If you're seeing this message, it means we're having trouble loading external resources on our website.
If you're behind a web filter, please make sure that the domains *.kastatic.org and *.kasandbox.org are unblocked.
To log in and use all the features of Khan Academy, please enable JavaScript in your browser.

Wireless Philosophy
Course: wireless philosophy > unit 6, euthanasia: why do people disagree about the ethics of euthanasia.
- Comprehending the argument
- Evaluating the argument
Want to join the conversation?
- Upvote Button navigates to signup page
- Downvote Button navigates to signup page
- Flag Button navigates to signup page
Video transcript
Home — Essay Samples — Social Issues — Euthanasia — Why Euthanasia Should Be Legal: Analysis of Arguments and Counterarguments
Why Euthanasia Should Be Legal: Analysis of Arguments and Counterarguments
- Categories: Assisted Suicide Euthanasia Right to Die
About this sample

Words: 1865 |
10 min read
Published: Aug 14, 2023
Words: 1865 | Pages: 4 | 10 min read
Table of contents
Introduction, why euthanasia should be legal, works cited, counterarguments.
- Corder, Mike. “Dutch Euthanasia Center Sees 22% Rise in Requests in 2019.” WAVY.com, 7 Feb. 2020, www.wavy.com/news/health/dutch-euthanasia-center-sees-22-rise-in-requests-in-2019/. Accessed 10 March 2020.
- Davis, Jacky. “Kevin Davis Deserved Choice.” Dignity in Dying, www.dignityindying.org.uk/story/kevin-davis/. Accessed 13 March 2020.
- De La Torre, Esther B. The Right to Assisted Suicide , www.lonestar.edu/rightto-assist-suicide.htm. Accessed 19 March 2020.
- “Euthanasia Laws - Information on the Law about Euthanasia.” Information on the Law about Euthanasia - Suicide, Life, Act, and Mercy - JRank Articles, law.jrank.org/pages/11858/Euthanasia.html. Accessed 10 March 2020.

Cite this Essay
Let us write you an essay from scratch
- 450+ experts on 30 subjects ready to help
- Custom essay delivered in as few as 3 hours
Get high-quality help

Dr Jacklynne
Verified writer
- Expert in: Social Issues

+ 120 experts online
By clicking “Check Writers’ Offers”, you agree to our terms of service and privacy policy . We’ll occasionally send you promo and account related email
No need to pay just yet!
Related Essays
1 pages / 670 words
6 pages / 2955 words
3 pages / 1531 words
3 pages / 1154 words
Remember! This is just a sample.
You can get your custom paper by one of our expert writers.
121 writers online
Still can’t find what you need?
Browse our vast selection of original essay samples, each expertly formatted and styled
Related Essays on Euthanasia
Euthanasia, a topic fraught with moral and ethical complexity, stands at the intersection of personal autonomy, suffering, compassion, and empathy. In this in-depth exploration, we will delve into the profound moral and ethical [...]
Euthanasia, also known as mercy killing, is a highly controversial topic that has sparked heated debates across the globe. The concept of euthanasia involves deliberately ending the life of a patient who is suffering from an [...]
Euthanasia, the act of intentionally ending a person's life to relieve their suffering, has been a topic of ethical debate for decades. This essay explores the nuanced and multifaceted arguments in favor of euthanasia, delving [...]
The debate surrounding euthanasia is complex and multifaceted, involving considerations of ethics, religion, personal autonomy, and the value of human life. While advocates argue that euthanasia provides relief to those [...]
Battin, M. P., Rhodes, R., & Silvers, A. (2015). The Patient as Victim and Vector: Can Ethics Abandon the Ideal of the Autonomous Patient? The American Journal of Bioethics, 15(3), 3-14.Pereira, J. M. (2011). Legalizing [...]
Imagine facing a terminal illness with no hope for recovery, only prolonged suffering and pain. In such situations, the concept of euthanasia, or assisted suicide, becomes a controversial but increasingly relevant topic. [...]
Related Topics
By clicking “Send”, you agree to our Terms of service and Privacy statement . We will occasionally send you account related emails.
Where do you want us to send this sample?
By clicking “Continue”, you agree to our terms of service and privacy policy.
Be careful. This essay is not unique
This essay was donated by a student and is likely to have been used and submitted before
Download this Sample
Free samples may contain mistakes and not unique parts
Sorry, we could not paraphrase this essay. Our professional writers can rewrite it and get you a unique paper.
Please check your inbox.
We can write you a custom essay that will follow your exact instructions and meet the deadlines. Let's fix your grades together!
Get Your Personalized Essay in 3 Hours or Less!
We use cookies to personalyze your web-site experience. By continuing we’ll assume you board with our cookie policy .
- Instructions Followed To The Letter
- Deadlines Met At Every Stage
- Unique And Plagiarism Free

The Ethics of Euthanasia
Malleeka Suy | SQ Blogger | SQ Online (2021-2022)
Picture t his: It is the year 3020, and the Martian soil you have been drilling into has finally worked out. Colonizing Mars is taking shape, and soon your family can permanently live on this rusty, rocky planet. However, the effects of progress don’t go unnoticed; every time you move, your skin screams in pain. Everything you once loved doing has lost its appeal. Would you take death in your own hands or live until a painful end?
This moral dilemma seems straight out of a science-fiction novel for most, but euthanasia is a legitimate deliberation for patients with terminal and mental illnesses who deem their lives too painful to live on. It is a practice that is still heavily debated in modern bioethics. Among many definitions, the American Medical Association defines euthanasia as the administration of a lethal agent by a medical professional to a patient to relieve their intolerable or incurable suffering.
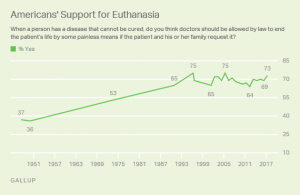
Although euthanasia is not a new scientific process, as it has been practiced since the time of the ancient Greeks more than three thousand years ago, it wasn’t generally accepted by Western medicine until recently. The Netherlands was the first country to allow legal euthanasia and assisted suicide in 2002, totaling 1.7-2.8% of total deaths. Euthanasia is generally illegal in the United States, but in a nationwide 2017 American poll , 73% of the public were in favor of euthanasia, and 57% said euthanasia is morally acceptable. These numbers are nearly double the initial poll in 1947. If I had to guess why, it may be partly because of progressive exposure to mental health and its effects. This may have allowed people to understand and empathize with the circumstances and support what euthanasia stands for: a release from an unbearable life.
Euthanasia is especially controversial among general society and the bioethical community. One main argument for the support of euthanasia is grounded in personal autonomy–our ability to act independently– since living life is about minimizing physical pain and maximizing dignity and control . This idea is rooted in ancient times when physicians considered dying with peace and dignity a human right. An article from Stanford’s Encyclopedia of Philosophy regards autonomy as self-determination, so choices about how and when people die is them taking responsibility for their lives. Terminally ill patients in Oregon mentioned how they chose euthanasia because their condition stripped them of their independence and ability to engage in activities that gave their life meaning. After all, what is the meaning of life if we cannot live it?
Another article by the Linacre Quarterly highlights how the ethics of compassion justify the use of euthanasia. From a humanitarian standpoint, we can show compassion by suffering and sympathizing with patients and respecting their wishes of euthanasia as their “remedy.” Kenneth L. Vaux, a consultant in medical ethics, notes in his article that physicians would give a lethal dose to their loved ones out of love if they were dying and suffering, so he finds it “strange and hypocritical” that doctors cannot legally do so for their patients. He claims that “we have lost empathy, sympathy, and the covenant of care with those who have entrusted their lives to us because they believe we embody those very qualities.” Vaux also asks: “Having barred the door to Death, are we not then obliged at some point to open it?” He suggests that since doctors bring life into the world every day, consensually ending a patient’s life for their benefit should be no different.
Despite popular social support, there are many arguments against euthanasia as well–the most popular being religion. Several faiths, such as Christianity, see euthanasia as a form of murder and find it to be morally unacceptable because it may weaken society’s respect for the sanctity of life. Religious groups actively argue against euthanasia, and for this reason, euthanasia became a debate of preservation and purity of life.
Even though medicine is rooted in science, some physicians also use religion as justification against practicing euthanasia. Contrary to public British opinion, studies show that most UK doctors do not support legislation permitting euthanasia due to their religiosity or faith, and less than a quarter of doctors would be willing to practice euthanasia if it became legal.
Physicians also have a professional obligation to fulfill that becomes morally blurred with euthanasia. For more than 2,500 years, doctors have taken the Hippocratic Oath to do no harm and treat those under their care. Does bringing death by euthanasia violate the Hippocratic Oath, or is it in line with a doctor’s mission? Would acting under Hippocrates then make a doctor a hypocrite?
Because of this subjectivity, doctors sometimes feel uncertain about administering euthanasia. Even if a patient is under a lot of pain and medication, how can doctors be sure that their decision was made rationally? In a Dutch article , an experienced psychiatrist dealing with a patient’s invisible suffering made him uncertain about assessing how deeply rooted their suffering really was, and therefore how moral it would be to allow euthanasia to happen. The fickle nature of the human mind makes many physicians and ethicists question whether or not euthanasia should be a normal practice.
Physicians often have their own reservations about euthanasia and how they cope with patients who wish for it. They frequently feel pressured by the patient or the patient’s relatives to perform euthanasia. A 2011 survey among Dutch physicians also found that 86% of physicians dread the emotional burden of performing euthanasia. One physician recounts how a patient told them, “If you won’t perform euthanasia, I might go to a railway line or climb a high building.” This form of blackmail can lead to dangerous expectations, where future normativity of the practice is anticipated or even praised.
Instead of placing the burden on doctors, what if the government or even robots could control euthanasia? Although this faceless jurisdiction seems like a good solution, critics argue that euthanasia would be normalized and twisted for eugenic purposes, adding to the nightmare of AI domination and impeding the sanctity and preciousness of life. These speculations seem inconceivable, but history has unfortunately seen it happen, such as in Hitler’s Germany, where Aktion T4, a Euthanasia Program systematically murdered patients with disabilities to restore the “integrity” of the German nation, thrived. Perhaps then a grimmer alternative to the use of euthanasia is the elimination of incurable, disabled, or elderly patients. Mechanization of euthanasia would also impact the patient and the medical profession, both in what it means to be human and obeying the Hippocratic Oath. Routinization of the practice could also increase the desires of people’s wishes to end their lives, whether individually justified or not.
References:
https://jamanetwork.com/journals/jama/article-abstract/2532018
https://plato.stanford.edu/entries/euthanasia-voluntary/#MoraCaseForVoluEuth
http://www.cirugiaycirujanos.com/frame_esp.php?id=308
https://www.sciencedirect.com/science/article/pii/S0885392414003066?via%3Dihub
https://www.healthline.com/health/what-is-euthanasia#making-a-decision
https://livinganddyingwell.org.uk/wp-content/uploads/2020/02/Redefining-Physicians-Role-in-Assisted-Dying.pdf
https://shibbolethsp.jstor.org/start?entityID=urn%3Amace%3Aincommon%3Aucsd.edu&dest=
https://www.jstor.org/stable/3561966&site=jstor
https://doi.org/10.1177%2F0269216310397688
https://www.medicalnewstoday.com/articles/182951#some-statistics
https://journals.sagepub.com/doi/10.1177/0269216310397688
https://www.nejm.org/doi/10.1056/NEJMclde1310667
https://medicine.missouri.edu/centers-institutes-labs/health-ethics/faq/euthanasia
https://news.gallup.com/poll/211928/majority-americans-remain-supportive-euthanasia.aspx
https://www.ama-assn.org/delivering-care/ethics/euthanasia
https://pubmed.ncbi.nlm.nih.gov/21145197/
https://doi.org/10.1016/j.jpainsymman.2014.04.016
https://www.ccsenet.org/journal/index.php/gjhs/article/view/19405/13366
https://encyclopedia.ushmm.org/content/en/article/euthanasia-program
- Search Menu
- Accident and Trauma
- Anaesthesia
- Cardiothoracic Surgery
- Cardiovascular Disease
- Child and Adolescent Psychiatry
- Critical Care/Intensive Care/Emergency Medicine
- Dermatology
- Endocrinology
- Environment and Disease
- Gastroenterology
- General Practice
- Geriatric Medicine
- Haematology
- Health Policy
- Health Economics
- Infectious Diseases
- Liver Disease
- Neonate Medicine
- Neurophysiology
- Neurosurgery
- Obstetrics and Gynaecology
- Occupational Medicine
- Ophthalmology
- Otolaryngology
- Paediatric Medicine & Surgery
- Palliative Medicine
- Perioperative Medicine
- Public Health Medicine
- Renal Medicine
- Respiratory Medicine
- Rheumatology
- Sports Medicine
- Transplantation
- Tropical Medicines
- Advance articles
- Editor's Choice
- Author Guidelines
- Submission Site
- Open Access
- About British Medical Bulletin
- Editorial Board
- Advertising and Corporate Services
- Journals Career Network
- Self-Archiving Policy
- Dispatch Dates
- Journals on Oxford Academic
- Books on Oxford Academic
Article Contents
The implication of a medicalized dying process, the historical case against physicians assisting suicide, the medical cloak, collaborators in euthanasia, healing and euthanasia, recent developments, is euthanasia medical treatment, acknowledgements.
- < Previous
Euthanasia is not medical treatment
- Article contents
- Figures & tables
- Supplementary Data
J. Donald Boudreau, Margaret A. Somerville, Euthanasia is not medical treatment, British Medical Bulletin , Volume 106, Issue 1, June 2013, Pages 45–66, https://doi.org/10.1093/bmb/ldt010
- Permissions Icon Permissions
The public assumes that if euthanasia and assisted suicide were to be legalized they would be carried out by physicians.
In furthering critical analysis, we supplement the discourse in the ethics and palliative care literature with that from medical education and evolving jurisprudence.
Both proponents and opponents agree that the values of respect for human life and for individuals' autonomy are relevant to the debate.
Advocates of euthanasia and assisted suicide give priority to the right to personal autonomy and avoid discussions of harmful impacts of these practices on medicine, law and society. Opponents give priority to respect for life and identify such harmful effects. These both require euthanasia to remain legally prohibited.
Proposals are emerging that if society legalizes euthanasia it should not be mandated to physicians.
The impact of characterizing euthanasia as ‘medical treatment’ on physicians' professional identity and on the institutions of medicine and law should be examined in jurisdictions where assisted suicide and euthanasia have been de-criminalized.
….tha'll nivver feel it, tha'll be out of existence i' two minutes
James Billington
Physician-assisted suicide (PAS) and euthanasia are among the most contentious issues faced by the medical profession. Numerous scholars have argued in favor of 1 or against 2 ‘assisted death’, as these interventions are euphemistically called. These debates generally take it for granted that the person carrying out euthanasia will be a physician. That assumption has been questioned, most recently, by two ethicists from the Harvard Medical School who propose a limited role for physicians in assisted dying. 3 We discuss their proposal shortly. The possibility of deleting the physician from the equation has certainly not been salient in professional discourse.
In this article we will examine factors, highlighting historical contexts and the influence of language, which have helped campaigners who aim to sanitize ‘assisted dying’ by associating it with medicine. We broach the issue of whether euthanasia can be considered medical treatment by focusing on the irreconcilability of euthanasia with medicine's mandate to heal.
In the remainder of this text, we use the word euthanasia to include PAS, unless the contrary is indicated. We do so in accordance with the fact that both procedures raise the same ethical and legal considerations with respect to many of the issues discussed in this article. In PAS and euthanasia, physicians and society are complicit in helping persons to commit suicide or giving them a lethal injection, respectively. Moreover, whether or not a society will alter its laws to allow ‘medically induced death’ is a binary decision.
Are medical doctors, by being responsible for the prolongation of the dying process, blameworthy for the existence of conditions that elicit a desire for hastened death? The profession has indeed created circumstances, through overly aggressive technical interventions, whereby persons' illness narratives have included chapters with alienating, depersonalizing and dehumanizing plots and characters. The following trajectory of a hypothetical patient with amyotrophic lateral sclerosis is all too common: first, non-invasive nocturnal ventilation enters the scenario; next, a wheelchair; then a Dobhof feeding tube, promptly replaced by a jejunostomy; innumerable venous punctures and catheterizations; intervening urinary tract infections; recurrent aspiration pneumonias, followed by invasive ventilation, eventually necessitating a tracheostomy; accompanied by unremitting despondency; and finally, progressive somnolence and terminal sepsis. Too many patients find themselves in a sickroom in such a state, one of spent physical resources and suspended hope or even total despair. Some would add that this metaphoric dwelling is also inhabited by a crushed spirituality.
Pro-euthanasia advocates sometimes present such scenarios to support their views that the profession is, in some measure, responsible for the condition in which a patient may conceive of no escape or redress other than self-willed death. A comment such as, ‘I'd rather die than slog on with deformity, disfigurement and disability', is not infrequently heard and, when expressed, often denounces a sequence of medical interventions rather than the original illness. In dire situations, one of the few avenues that can seem to offer a sense of comfort is that of personal control. Control, usually packaged in a discursive frame of politico-judicial personal autonomy, can be manifest as a desire to manage the ultimate mode of exit from life, that is, for patients to select the method, place and hour of their death. Moreover, some may want this stance to be legitimized by societal approval and even see it as a heroic act and as furthering a common cause, by promoting shared values and ideologies. 4
It would, however, be an overstatement to attribute all changes in the nature of death to the health professions. Improvements in general socioeconomic conditions have decreased the incidence of death from catastrophic accidents, trauma and obstetrical mishaps and have lessened the impact of previously deadly infectious diseases. Undeniably, the shift in prevalence from acute and preventable conditions to chronic degenerative diseases, as well as many cancers, is a consequence of a prolongation of life resulting from improvements in public health, universal literacy and preventive interventions. Nonetheless, there is a kernel of truth in the notion, expressed in commentaries dating from Hellenistic to modern times, that physicians have invented ‘lingering’ death. 5 We believe that some of the profession's approaches in responding to illness in modern society may have fueled the clamour for radical solutions such as euthanasia.
The process has been abetted by those who espouse so-called ‘progressive values’, in what are often referred to as the ‘culture wars’, and who often manifest a pervasive questioning of authority. 6 A desire for unfettered individual decision-making powers—seeing ‘radical autonomy’ as always being the overriding value—and the demotion of established religions as influential voices in the public square are also important factors in the rise in demands to legalize euthanasia. We consider euthanasia a misguided solution to a complex socio-cultural transformation. It is reasonable that the medical profession not deny its contributions to the situation; but, it would be perverse if it allows itself to be co-opted by a perceived need for atonement. It must be vigilant to avoid over-compensating by endorsing society-sanctioned euthanasia.
The profession must not disown its ethical tradition or abandon its basic precepts. The potential harm is not only to individuals, but also to the institutions of medicine and law and the roles they play in society, especially in secular societies, where they are the primary carriers of the value of respect for human life, at the level of both the individual person and society. Ironically, they are more important in this regard now than when religion was the main carrier of the value of respect for life. 4 Therefore, the degrees of freedom, in terms of legitimate actions and behaviours available to physicians confronted with a dying patient are, and must remain, clearly and strictly limited.
The injunction against physician involvement in hastening death has recurred throughout recorded history, the Hippocratic Oath providing the following emblematic statement: ‘I will neither give a deadly drug to anybody if asked for it, nor will I make a suggestion to this effect’. 7 This unambiguous prohibition has oriented medical practice towards specific ends and means and away from certain others for over 2400 years. Its enduring impact was apparent in early-modern Western society. Euthanasia was discussed by the lawyer Casper Questel in a book entitled ‘De pulvinari morientibus non subtrahendo’. 8 Translated as ‘On the pillow of which the dying should not be deprived’, it described common practices that were thought to hasten death. These popular practices included removing pillows from dying persons so that, with their bodies completely supine, ventilatory capacity would be constricted and death accelerated. Another strategy was to transfer dying persons from their beds to the ground. Perhaps the latter operated through a tacit understanding that the bodily cold thereby induced would bring dying persons closer to their natural demise. Regardless of the underlying pathophysiologic mechanism, it is highly probable that symbolism (for example, facilitating passage of the soul from the shell of the dying body to life eternal) was at play. We note that it was natural death that was sought, not terminating the life of the person.
An intriguing and noteworthy feature of this ancient text is that such practices were popular amongst the general public. They were not acts delegated by society to a particular group and certainly not restricted to medical doctors. Questel was aware of undesirable ramifications if they were practiced by physicians. Physicians risked losing trust should they be discovered to have intentionally shortened the lives of dying patients. Trust is of paramount importance to a successful doctor–patient encounter and is indispensable to the implicit moral contract between the profession and society. 9 Maintaining the trust of individual patients and of society is a sine qua non for the maintenance of professional status. Participating in euthanasia carries the risk of vitiating trustworthiness.
Constraints on physician complicity in euthanasia are to be found throughout history. An 1826 Latin manuscript by a physician, Carl Friedrich Marx, referred to medical euthanasia as the skillful alleviation of suffering. 10 He absolutely forbade physicians from engaging in any attempt at accelerating death, stating : ‘ … and least of all should he be permitted, prompted either by other people's request or his own sense of mercy, to end the patient's pitiful condition by purposefully and deliberately hastening death’. Examples of more recent statements of such prohibitions include the defeat in the House of Lords in 1932 of the ‘Voluntary Euthanasia Bill’ 11 and the Canadian parliament's clear rejection in 2010, by a vote of 228 to 59, of Bill C-384, a private member's bill that would have permitted PAS and euthanasia. 12
Certain jurisdictions, notably the Netherlands and Belgium, have legalized euthanasia. In America, Oregon's ‘Death with Dignity Act’, which permits PAS, came into force in 1997 and Washington state followed suit in 2008. However, on 6 November 2012, Massachusetts voters defeated a ballot that would have allowed assisted suicide, 51–49%. There have been discussions, debates and proposed legislation in many other American states and other countries in the recent past. Generally, these have reaffirmed the ban on medical assistance in killing (whether in the context of end-of-life or, in the USA, physicians' involvement in carrying out capital punishment through lethal injections). The Benelux and a few American states represent the exception to the rule. ‘Do not kill’ has been considered a moral absolute for most physicians for millennia, and remains so for physicians even in jurisdictions where the public has looked favorably on legislative change. That medicine has all to do with healing, and nothing to do with the purposeful ending of life, has been a reverberating imperative throughout history.
The pro-euthanasia lobby derives advantages by aligning itself tightly with medicine and physicians. The history of physician involvement in capital punishment is illustrative of this strategy. Juries in the USA, who had seen horrific footage of convicted murderers being executed in the ‘electric chair’, became reluctant to convict persons accused of capital offences or to vote for a death sentence for felons convicted of a capital offence. Most physicians and the American Medical Association adamantly opposed medicine's involvement in administering capital punishment by lethal injections. Nevertheless, some physicians participated. By virtue of their involvement and in concocting a method of execution that makes a convicted criminal appear serene during final moments, enhanced acceptability was conferred on the procedure. It has been suggested that ‘the law turned to medicine to rescue the death penalty’. 13
It is germane to point out that the word ‘doctor’ is linked etymologically to ‘teacher’. The Oxford English dictionary's definition is: ‘one who gives instruction in some branch of knowledge, or inculcates opinions or principles’. 14 Medical doctors can influence public opinion, much as teachers contribute to the socialization of their pupils. The recruitment of doctors, both as a collectivity and as individuals, to undertake a procedure, can greatly modify the public's view of that procedure.
Language is critically important in not only reflecting, but also creating reality. For example, the field testing conducted prior to the passage of the Oregon Death with Dignity Act demonstrated that when the intervention was described as ‘suicide’ or ‘euthanasia’, popular support declined by 10–12%. 15 The phrase ‘death with dignity’, by avoiding the negative connotations of suicide, was perceived as less alarming. It was able to create a halo of benignity and to generate greater support for and muted opposition to the proposed law. For similar reasons, the euphemism ‘physician assistance in a dignified death’ is reassuring. It would be rare indeed for an individual to wish explicitly for a gruesome death or want to banish a benevolent healer from the sickroom. Research shows that emotions, 16 which we would qualify as ‘examined emotions’, and we would add, moral intuition, are important in making good ethical decisions. Choice of language affects both these human ways of knowing what is morally right and morally wrong. 17
Jill Dierterle, a member of the Department of History and Philosophy at Eastern Michigan University, denigrates the validity and power of words in order to claim that none of the anti-PAS arguments hold merit and concludes that ‘we have no reason not to legalize it’. 18 She turns a blind eye to any potential harm and conveniently overlooks the lacuna in current data-gathering procedures or impact assessments. This stance flies in the face of the golden rule of medicine: primum non nocere. Hence, it is anathema to the vast majority of practicing physicians. Few of us, presented with a new and relatively untested therapeutic instrument, would conclude, ‘we have no reason to doubt its safety; let's forge ahead’. Her nonchalant dismissal borders on the offensive. Note how she handles an important deontological argument against PAS: ‘ … if PAS is wrong, its wrongness cannot be constituted by its conflict with the Hippocratic Oath. After all, the Hippocratic Oath itself is just a bunch of words’. 18 With the phrase ‘just a bunch of words’ Diertele implies that the oath is hollow and meaningless. But ethical precepts and laws are also just a ‘bunch of words’, yet they establish our metaphysical reality—what can be called our metaphysical ecosystem—which, depending on its nature, determines whether or not we have a society in which reasonable people would want to live.
It is critical to the euthanasia debate to consider what role, if any, physicians may, should or must not play. It is not a ‘given’ that, were euthanasia to be legalized, it would be inextricable from the medical mandate. We propose that it is in the best interests of individuals and society to remove the medical cloak from euthanasia in order to lay bare fundamental arguments against it. The stakes are too high to have the veneer of doctoring obscure the essential core of what is involved and its potential harms and risks.
The commentary previously mentioned, ‘Redefining Physicians’ Role in Assisted Dying’, suggests that a non-physician group could be made responsible for the ‘active’ role in euthanasia. 3 The label ‘thanatologist’ has been suggested for such a group. 11 The possibility that a new discipline might emerge raises a set of intriguing questions: What would be the scope of practice of thanatologists? Where would one draw the line between ‘active’ and ‘passive’ roles? Of what might their education consist? We want to make it clear that we believe euthanasia is inherently wrong and, therefore, should never be undertaken, but, it is important to consider what such a proposal could involve if it were put into practice.
It is reasonable to speculate that the training could be offered in a program at a technical level and that the duration of training period would be modest. The act of terminating someone's life is thought to be fairly straightforward—at least, the execution of it is not overly complicated. The experience in the UK of recruiting and training hangmen can provide useful clues. 19 Executioners were trained in the late 19th to mid-20th century with a 5-day course that included lectures, a practical component—‘applicants to pass pinioning in the presence of the Governor’—and ended with a written examination that included simple algebra—the applicant was required to calculate the length of drop (i.e. stretch of the rope) for men of varying weights. Given the complexity of drug-based protocols used in euthanasia, 5 days of instruction would likely be insufficient. A program in the order of 24 weeks, as is the case for cadet training in many police academies, might allow for core objectives to be adequately covered and relevant abilities to be tested and credentialed.
A provocative essay on the topic suggests that lawyers could be trained in euthanasia, practicing a new specialty called legistrothanatry. 20 Although admittedly implausible, the proposal serves to foreground pragmatic issues relevant to the debate. It rests on two fundamental assumptions: (i) that lawyers are trained to interpret laws and regulations accurately, to apply them strictly and to act on the basis of implementing patients' values and (ii) that carrying out the required tasks does not require sophisticated technical expertise. The authors state, ‘Attorneys who wish to provide this service would require only a small amount of additional training’. 20 An appropriate educational blueprint could include the following cognitive base: the physiology of dying, basic pharmacology and an overview of the historical, ethical and legal aspects of natural and requested/assisted death. The toolkit of required skills would likely include: communication, verification of decision-making capacity and informed consent, securing of intravenous access, supplying and/or administering of lethal drugs, management of complications, accurate recognition of death and completion of death certificates. The desired attitudinal substrate would include: personal resolve (that is, stick-with-it-ness), respect for individuals' rights to autonomy and self-determination, and, ideally, a calm demeanour.
Although the tone of the previous discussion may be—and should be—rather ‘chilling’, the substance it addresses has clearly gained a foothold in the current medical literature. A description of procedures for successful euthanasia has been published; one is entitled ‘Euthanasia: medications and medical procedures’. 21 It includes protocols for dealing with terminal dyspnea or agitation in the terminal phase, euthanasia, and the induction of ‘controlled sedation’. Controlled sedation is placed in inverted commas by the author, presumably because he feels that it needs qualification; in his opinion, it represent a hypocritical response to suffering and is undertaken with the aim of muzzling the patient while he dies. We note, but will not discuss here, the ethical issues raised by ‘palliative sedation’, sometimes called ‘terminal sedation’, in which the dying patient is sedated in order to relieve otherwise unrelievable suffering. We suggest that the former term should be used when sedation is the only reasonable, medically indicated, way to relieve the patient's suffering (when it is not euthanasia); the latter term is appropriate when those conditions are not fulfilled and the doctor's intention is to hasten the patient's death (when it is euthanasia).
The epigram to the euthanasia guidelines cited above is fascinating. It states: ‘One summer evening, Mr J-M L, suffering from Charcot's Disease, passed away peacefully after having asked for and obtained the assistance of a physician. Upon leaving the home, the latter did not ponder: ‘What did I do?’ but rather, ‘Did I do it well?’ (Translation by author JDB) 21 This formulation reveals a unique mindset. The affective and moral stance expressed in that quote is closely aligned to a technical perspective, one where the emphasis is on accomplishing tasks with self-efficacy as opposed to one embellished with critical reflection. Meta-reflection is an important aspect of doctoring. What we do and the conversations we routinely engage in forge who we become; they become a habitus. Even the clothing we wear can influence our thought processes. For example, a recent article documents the impacts on cognition of donning a lab coat. 22 If the simple habitual act of wearing a white lab coat can affect thinking and action, one can easily imagine the harmful impacts of regular discussions of euthanasia as they insinuate themselves into the ethos of medical care.
‘The Executioner's Bible’, a story of England's executioners in the 20th century, describes the work of the hangman as a ‘cold, clinical operation’. 19 The epigram we have chosen for our essay, extracted from that textbook, is a quote from James Billington, the UK's Chief Executioner from 1891 to 1901. It is intended to evoke calculated efficiency. The author of ‘Euthanasia: medications and medical procedures’ is similarly categorical, prescriptive and unrestrained by self-doubt. For example, he advises the physician not to propose suicide without medical assistance; to do so is considered incompatible with the role of the physician. He warns the physician against using ‘violent options’ (such as injecting potassium chloride) as this is considered contrary to medical ethics. Leaving aside a disregard for the value of respect for life, the punctilious euthanizer can be seen as behaving with professional dignity and serenity, within a priori defined limits. As the Home Office stated in 1926, when describing the work of hangman William Willis, ‘ … .even an executioner can remain humane and decorous’. 19 Our purpose in making this historical link is not to denigrate advocates of euthanasia. Rather, through this analogy we are endeavoring to focus on the act itself and not just the actor. The latter is often well meaning.
Thanatologists, given the narrow focus of their field of expertise would, over time, almost certainly develop clinical practice guidelines; these might be tailored to different illness categories, for instance, neurodegenerative diseases and the various cancers with poor prognosis. This process seems to be well underway. For example, a recent paper explores euthanasia requests and practices in a highly particularized context, namely, patients in Belgium dying of lung cancer. 23 If euthanasia is accepted as integral to ‘medical care’, this sort of disease-specific focus will surely expand. One can envisage the emergence of guidelines delineating the complementary roles of physicians and thanatologists. Most physicians (we hope) would eschew any involvement in euthanasia and confine themselves to traditional roles such as diagnosing, estimating prognosis and providing supportive care and symptom control, that is, excellent palliative care—which does not include euthanasia, as some advocates argue it should.
The extent to which principled opponents of euthanasia would be legally ‘excused’ from participating in the steps leading up to fulfilling a patient's request for assisted death is a contentious aspect of the debate. How would the profession balance the requirement for individual physicians to fulfill specific social roles and the need to respect the freedom of conscience of those who, on moral grounds, reject certain options? Physician–philosopher Edmund Pellegrino argues that physicians can refrain from entering into professional relationships that have the potential to erode their moral integrity; he offers strategies to assist the physician in navigating potential conflicts. 24
Psychiatrists and medical ethicists who do not reject euthanasia would be expected to focus on soliciting patient perspectives, exploring options and assessing comprehension, competence and voluntariness—that in making her decision, the patient is free from coercion, duress or undue influence, assuming this is possible. The profession has begun to equip itself with tools to deal with this incipient new clinical reality in jurisdictions which allow euthanasia. Physicians in the USA have been provided with an eight-step algorithm to assist them in discussing assisted suicide with patients who request it. 25 These guidelines were developed immediately after the legalization of PAS in Oregon. It is reasonable to expect that additional decision-making tools will emerge should the practice gain wider societal acceptance. Also, the possible consequences on undergraduate medical education, should it have to include protocols for ending patients' lives, have been explored. 26
Again, we note that the above discussion is included for the sake of comprehensive coverage of the issue of physicians' involvement in euthanasia, were it to be legalized, and whether it could be ethically acceptable ‘medical treatment’ or even ‘therapy’. It is not meant to signal that we see euthanasia as ethically acceptable.
It has been repeatedly found that of all separately identified groups in Western societies, physicians are among the most opposed to involvement in euthanasia. There is substantial indirect evidence to support this claim, even in jurisdictions in which doctor-assisted death is legal. For example, in Oregon, there is a suggestion that some patients have to resort to ‘doctor shopping’ to obtain their lethal medications. The Oregon Public Health Division's annual report for 2011 shows that one physician was responsible for 14 of the requisite prescriptions out of a total of 114 that year. 27 Also, the Netherlands recently approved the launching of mobile euthanasia clinics. A stated reason for this development was that patients' goals in self-determination were being thwarted by physician resistance to providing euthanasia. Not all physicians, including many Dutch colleagues, are on-side with having euthanasia become a medical act.
A questionnaire-based study comparing the opinions of the Dutch general public with that of physicians revealed some marked differences. With respect to the active ending of life for patients with dementia, the level of acceptance was 63% for the public and 6% for physicians. 28 With respect to terminally ill cancer patients, the figures were much higher and less divergent; this may be a consequence of the prolonged experience of euthanasia in cases of terminal illness in the Netherlands. Or, it might be that often survey questions are phrased as, ‘If a person is in terrible pain, should they be given access to euthanasia?’ The respondent must choose between leaving the person in pain and euthanizing them. But this choice is wrongly constructed. The person should be able to choose fully adequate pain management—that is, the ‘death’ of the pain—without having to endorse the intentional infliction of death on the patient. 29 Despite high levels of acceptance by physicians of euthanasia for cancer patients in the Netherlands, recent reports reveal persistent ethical concerns. 30 It is also noteworthy that physicians involved in palliative care, including in Britain, appear to be particularly concerned about legalizing euthanasia. 31
What underlies the medical profession's reluctance to accept euthanasia? There are multiple explanations. Aside from ethical, moral and religious beliefs, one of the most salient and compelling has to do with one's conception of the medical mandate, especially as it relates to healing. Healing is a challenging term to define. Many in our institution (the Faculty of Medicine, McGill University) consider it to be ‘a relational process involving movement towards an experience of integrity and wholeness’. 32 It has been operationally defined as ‘the personal experience of the transcendence of suffering’. 33 A feature of healing important to our thesis is the notion that healing does not require biological integrity. Although it may seem counter intuitive at first glance, it has been pointed out that if a sick person is able to construct new meaning and is able to achieve a greater sense of wholeness, that individual may ‘die healed’. 32 It is undeniably a vastly different concept than curing, although they are not in opposition one to the other. Most physicians accept the healer role as a fundamental and enduring characteristic of the profession. 34 In our undergraduate medical program, this concept is taught using the term ‘physicianship’; it refers to the dual and complementary roles of the physician—the physician as healer and professional. 35 It could be argued that one can remain ‘professional’ even while serving as a collaborator in requested death. On the contrary, many commentators—the American Medical Association is a prime example 36 —believe that it is impossible to do so as a ‘healer’, one who is focused on accompanying the patient on a transformational journey towards personal integrity that transcends the embodied self.
The process of healing in the doctor–patient relationship is poorly understood. We do not have a complete picture of how it is initiated or which clinical skills or abilities are essential in fostering a healing relationship. The literature suggests that healing resides in the quality of interpersonal connections and that it requires a deep respect for the agency of the physician in the therapeutic process. 37 An appreciation of the placebo effect, or in more poetic terms, the ‘doctor as the medicine’, is required. 38 , 39 It is almost certainly linked to the phenomena of transference and counter-transference and it may utilize the power differential for salutary purposes, even if these phenomena operate largely at a covert level.
The patient–doctor relationship is marked by intense ambivalence. Any physician who has initiated a discussion with a patient on the issue of resuscitation or desired level of technical intervention will realize how easily it can be misinterpreted, how quickly it can catalyze existential angst and how thoroughly it can overwhelm hopeful sentiments. Affective turmoil and cognitive dissonance can rapidly ensue. These sorts of cross-purpose exchanges would surely be magnified in the context of discussions regarding euthanasia. Although there may be a productive ‘meeting of the minds’ in any specific doctor–patient dyad, the risks of emotional derailment, self-effacing dependency and irremediable miscommunication should not be minimized. It is inconceivable to us that deep layers of existential suffering would not be activated and exposed by such a discussion. A healing space that can support patients would be unnecessarily deflated. Admittedly, this belief is based on incomplete understandings of the clinical encounter, yet the axiomatic foundation of that encounter is anchored in a 2400-year old tradition. We must consider why we have so jealously guarded that tradition. We could always have abandoned it by accepting euthanasia. Unlike many other current medical–ethical dilemmas, neither death nor euthanasia is a novel issue presented by new technoscience.
Many proponents of euthanasia like to claim that opponents rely on two types of unsound arguments: one based on empirical data and the other anchored in axiology. In the first instance, they allege that the outcomes data available from jurisdictions where euthanasia or assisted suicide has been legalized, suggest that our fears of potential abuse are groundless. They deny that there is a ‘logical’ slippery slope—that the situations in which euthanasia will be available will expand over time—or a ‘practical’ slippery slope—that euthanasia will be used abusively. Pro-euthanasia advocates claim that evolving legislation does not pose a threat to persons with a disability, does not lead to euthanasia without consent, does not invite extension of the practice to vulnerable populations—in short, that it has not become a ‘run-away train’. They usually express satisfaction with individual clinicians' professional restraint and integrity as well as with administrative safe guards. Some suggest that the acceptance of euthanasia results in improvements in traditional palliative care. This belief that it represents a positive force for changing prevailing clinical practices is not based on robust evidence. Moreover, the evidence for the existence of a practical slippery slope is very convincing. This was very recently affirmed by the High Court of Ireland, in a judgment we discuss shortly, in deciding whether prohibiting assisted suicide contravened the Irish Constitution, which it held it did not. 40
A recent dramatic example of the logical slope's gravitational pull is the euthanizing, in December 2012, of 45-year-old twins in Belgium. Deaf since childhood, Marc and Eddy Verbessem were facing the additional disability of blindness. Accepting that they were irremediably suffering, their physician euthanized them. 41 Euthanizing patients with non-terminal conditions, even though it can be legal in Belgium, will surely meet with the disapproval of most physicians. Even within the pro-euthanasia movement, this development may be considered an aberration. Nonetheless, there are increasing numbers of commentators who subscribe to the following philosophy: ‘If a patient is mentally competent and wants to die, his body itself constitutes unwarranted life-support unfairly prolonging his or her mental life’. 42
There are two arguments, both warranting careful scrutiny, frequently advanced in support of physician involvement in euthanasia. The first is that physicians have privileged access to information about their patients' unique perspectives and circumstances, including personal resources and frailties, as well as complex family dynamics. That argument has been undermined by evolving practices. The ‘Oregon Public Health Divisions’ report for 2011 reveals that the median length of the doctor–patient relationship for those who died by PAS was merely 12 weeks (with a range of 1–1379 weeks). 27 It is highly unlikely that a physician would have acquired a sophisticated understanding of a person's values, hopes and fears in the matter of a few weeks. It is even less plausible in the case of the mobile euthanasia units currently being deployed in the Netherlands. The second argument is that physicians are inclined, by temperament and experience, to accompany their patients throughout the illness trajectory, including death. That too is not defensible on the known facts. For example, in Oregon, in the first 3 years of the administration of Oregon's ‘Death with Dignity Act’, physicians were present at approximately half of assisted deaths. By 2005, it was 23%. In 2011, it was a mere 9%. 27 The behaviour of these prescribing physicians is not congruent with the image of physicians represented in that iconic painting by Sir Luke Fildes, bearing the title ‘The Doctor’, and often used to portray empathic witnessing. Pro-euthanasia advocates can come across as rather intrepid in their defense of personal autonomy. Autonomy is the overriding principle that is used to buttress arguments in favor of euthanasia; indeed, it generally runs roughshod over all other considerations. Many pro-euthanasia commentators are disposed to brush off concerns about the impact of accepting ‘radical autonomy’ as always being the overriding value—especially concerns about the risks and harms to vulnerable people and to important shared values, in particular, respect for life at the societal level. A 2012 case in British Columbia manifests all these issues; it involved vulnerable persons, values conflicts and shows the preferencing by the court of the value of individual autonomy in relation to euthanasia. The case originates in a challenge to the Canadian Criminal Code's current prohibition of assisted suicide. 43
Gloria Taylor, a plaintiff in the case, Carter v Canada (Attorney General) 44 , was a person with ALS who requested assisted suicide arguing that as her illness progressed she would be incapable of committing suicide, unaided, due to her physical disability. The judge, Justice Lynn Smith, ruled in the plaintiff's favour on the basis that the prohibition was unconstitutional on the grounds that it contravened both Ms Taylor's constitutional ‘right to life, liberty and security of the person’ (under section 7 of the Canadian Charter of Rights and Freedoms) 45 and her right not to be discriminated against as a physically disabled person (under section 15 of the Charter ); and that the prohibition could not be saved (under section 1 of the Charter ), as a reasonable limit on constitutionally protected rights. Consequently, the judge held that the law prohibiting assistance in suicide was not applicable with respect to preventing Ms Taylor and other people in similar circumstances from having such assistance. The judgment is very long and legally complex and is now on appeal. Read as a whole, it strongly supports legalizing PAS and euthanasia.
In that case, the Canadian court reviewed the available evidence from other jurisdictions with liberalised legislation and concluded that there was no evidence of abuse. This Court also reviewed the same evidence and has drawn exactly the opposite conclusions. The medical literature documents specific examples of abuse which, even if exceptional, are nonetheless deeply disturbing. Moreover, contrary to the views of the Canadian court, there is evidence from this literature that certain groups (such as disabled neonates and disabled or demented elderly persons) are vulnerable to abuse. Above all, the fact that the number of LAWER (‘life-ending acts without explicit request’) cases remains strikingly high in jurisdictions which have liberalised their law on assisted suicide (Switzerland, Netherlands and Belgium) – ranging from 0.4% to over 1% of all deaths in these jurisdictions according to the latest figures – without any obvious official response speaks for itself as to the risks involved’. 40
One can also question Justice Smith's conclusions that PAS is not inherently unethical; that individuals' right to autonomy takes priority over the value of respect for life; that sanctity of life is only a religious value; that there is no relevant ethical or moral difference between refusals of life-support treatment that result in the death of the patient and euthanasia; and, that the availability of legalized PAS is necessary ‘medical treatment’ for some.
Justice Smith's justification for allowing euthanasia is largely based on a selective application of Canadian Charter of Rights and Freedoms jurisprudence 45 and depends upon her being able to distinguish the binding precedent set by the Supreme Court of Canada in the Rodriguez case. 46 The latter held, in a four to three split among the judges, that the Canadian Criminal Code's prohibition on assisted suicide 43 was constitutionally valid.
Invoking the Canadian Charter of Rights and Freedoms , Justice Smith ruled that Ms Taylor's right to life was infringed by the prohibition of assisted suicide because she might conclude that ‘she needs to take her own life while physically able to do so, at an earlier date than she would find necessary if she could be assisted’. 44 We believe that this would strike many as a straw man argument. It is to convert a right to life to a right to assisted suicide, by accepting as a breach of a right to life that a person will commit suicide sooner, if not given access to assisted suicide. But validating assistance in committing suicide hardly upholds a right to life.
Like everybody else, Ms Taylor has a right to refuse treatment even if that means she will die sooner than she otherwise would. Justice Smith accepts the plaintiffs' argument that there is no ethical or moral difference between euthanasia and refusals of life-support treatment that result in death and, therefore, both should be legal. But a right to refuse treatment is based in a right to inviolability—a right not to be touched, including by treatment, without one's informed consent. It is not a right to die or a right to be killed. At most, people have a negative content right to be allowed to die, not any right to positive assistance to achieve that outcome. A person with Ms Taylor's illness trajectory will surely die—even more precipitously if they decline many of the interventions described in the hypothetical patient with ALS we introduced earlier on. (Subsequent to the judgment, Ms Taylor died a natural death from an infection). It is also important to underline that current medical practices enable physicians to attenuate much of the suffering that may accompany the progressive loss of function and well-being in advanced ALS.
The judge appears also to accept the argument that legalizing euthanasia enhances palliative care. This goes some way towards treating euthanasia, as some have termed it, ‘the last act of good palliative care’. 47 It is also consistent with the ‘no-difference-between-them approach’ to a spectrum of end-of-life medical interventions. Euthanasia is confused with interventions, such as pain management and rights to refuse treatment, which are ethically and legally acceptable, and an argument is thus set up that, if we are to act consistently, euthanasia must also be ethically and legally acceptable. It is tantamount to legalizing euthanasia through confusion. 48
In the policy, ‘palliative care’ is defined as ‘a qualified medical practitioner, or a person acting under the general supervision of a qualified medical practitioner, administering medication or other treatment to a terminally ill patient with the intention of relieving pain or suffering, even though this may hasten death’. The policy states that that conduct, ‘when provided or administered according to accepted ethical medical standards, is not subject to criminal prosecution’. 44
In other words, the policy's definition of palliative care can be expansively interpreted to place euthanasia in same category as other end-of-life interventions which may hasten death.
For the sake of exploration of the issue, let us assume momentarily that euthanasia is medical treatment. What might flow from this?
Classifying euthanasia as medical treatment would affect the scope of disclosure of information necessary to obtain informed consent. A physician must disclose to the patient all reasonably indicated medical treatments as well as their risks and benefits. It would now have to include euthanasia. Even most pro-euthanasia advocates regard it as unethical for a physician to introduce the possibility of euthanasia. Currently, it is generally accepted that any discussion of it must be initiated by the patient.
It would also mean that to obtain informed consent to euthanasia, all reasonably indicated treatments would need to be offered and they would certainly include all necessary palliative care, in particular, fully adequate pain management. Many of those advocating for euthanasia posit euthanasia and palliative care as alternatives, but informed consent to euthanasia could not be obtained unless good palliative care was available. This is not available to a majority of people who die in Canada; it has been estimated that less than 30% have access to even the most minimal form of palliative care. 49
As well, Canadian psychiatrist Dr Harvey Max Chochinov, who specializes in psychiatric treatment for dying people, has shown that there are significant fluctuations in the will to live, even as death is imminent. 50 The impact of these findings, as well as conditions such as depression, on the possibility of obtaining valid informed consent to euthanasia would need to be fully addressed.
Another crucially important issue is that, if PAS and euthanasia are ‘medical treatment’, then surrogate decision-makers have the authority to consent to them for the patient. Their decisions must be based on either their knowledge of what the patient would have wanted or, if those wishes are unknown, their belief that these interventions are in the ‘best interests’ of the patient. Would mentally incompetent people and those with dementia or disabled newborn babies, as is now the case in the Netherlands under the Groningen protocol, be eligible for ‘therapeutic homicide’? 51
Yet another issue is what would be the indications for euthanasia as medical treatment and who could access it if were legalized? Justice Smith, citing an expert witness for the plaintiffs, refers to ‘the end-of-life population’. 44 This is a term used in the Royal Society of Canada Expert Panel Report on End of Life Decision - Making. 52 In the report, this population is defined as those persons on a continuum beginning with any serious diagnosis or injury. This represents an expansion of a term, ‘end-of-life’, traditionally used for those inevitably in the last days of life, to all people with serious chronic conditions, resulting from illness or injury, that may be fatal in the course of time. And, of course, it is notoriously difficult to predict with any certainty the timing of even obviously terminal illnesses. It is precisely the type of ‘slippery slope’ that we fear emerging from the ‘limited’ exception, as defined by Justice Smith. It will likely culminate in more decisions similar to that taken in the case of the Verbessem brothers in Belgium.
It is also pertinent to point out that Canada continues to fund and promote programs that aim to prevent suicide. If suicide is conferred the status of a right or is held to be acceptable medical treatment it would be difficult to reconcile this situation with the presence of programs that aim to actively thwart it. Some resolve this dilemma by trying to banish the word ‘suicide’ from the debate, in favor of the phrase ‘assisted dying’. Marcia Angell, erstwhile editor of the NEJM and a fervent proponent of PAS, endorses the notion that ‘assisted dying’ can be distinguished from ‘typical suicide’. The latter is described as being undertaken by someone with a normal life expectancy, whereas the former is carried out in someone ‘who is near death from natural causes anyway’. 53 They are going to die anyway, so what does it matter?! We believe that this reasoning is rather disingenuous and that it can result in a dishonouring of that segment remaining in someone's life, whether this is measured in minutes or months, and could deprive them of something as ephemeral as dreams and hopes. It certainly negates the idea of dying as our last great act of living. 54
Finally, a decision classifying euthanasia as medical treatment could have impact far outside the context of issues directly related to death and dying. For example, in Canada, the federal and provincial governments' respective powers are allocated under the Canadian Constitution. The criminal law power belongs to the federal parliament and the power to govern health and social services to the provincial legislatures. If euthanasia was defined as medical treatment, the federal parliament's prohibition of it in the Criminal Code could be invalid by reason of its trespassing on the provincial jurisdiction to govern health and social services. That is one reason that the Quebec College of Physicians and Surgeons, which supports legalizing euthanasia, argues that it is medical treatment. Likewise, the Quebec Legislative Assembly committee, which issued a report, ‘Dying with Dignity’, 55 adopts the same argument. From past experience, we expect that Quebec might challenge the constitutional validity of the Criminal Code prohibition on this basis. However, a legal committee, set up by the Quebec government, has proposed another approach. It has just reported on how Quebec could operationalize giving doctors legal immunity for carrying out euthanasia, including by the Attorney General of Quebec instructing Crown Prosecutors not to prosecute them under the Criminal Code for doing so, provided they comply with certain guidelines. 56 In either case we could see Quebec becoming ‘separate’ from the rest of Canada on this critically important issue.
In pondering medicine's possible involvement in euthanasia, we must foreground those aspects of the medical mandate that are immutable and eternally relevant. We believe these to be the constant nature of ‘illness’, changeless across time, place and culture, and the resultant obligations of the healer. It is important to appreciate how illness affects persons in all spheres of their lives. Patients become intensely vulnerable, impressionable and open to abuse. Pellegrino has summarized the nature of the clinical encounter eloquently as ‘a peculiar constellation of urgency, intimacy, unavoidability, unpredictability and extraordinary vulnerability within which trust must be given’. 57 This vulnerability sets up an intense and enduring obligation of physicians; they must respond to the wounded person with authenticity, compassion and moral agency. The latter demands that physicians harness and deploy their unique influences and persuasive powers in a particular manner. The essential nature of physicianship has evolved over time in a direction that recognizes the extraordinary vulnerability of patients and guards ferociously against their exploitation. In part, this has been achieved by imposing inviolable limits on the physician's terrain of action. Moreover, we believe that, even if one accepted that euthanasia was ethically acceptable—which we do not—it opens up too many doors for abuse.
The medical profession has arrived at a crossroad; it must choose whether to embrace euthanasia as medical treatment, as a logical extension of end-of-life care, or it can reject the redefinition of its healing mandate that this would entail. We believe, that looking back in the future, the euthanasia events of the present time will be seen as a turning point, not only for the profession of medicine, but also for societies. Crossing the line in the sand articulated by Hippocrates, that as a physician ‘I will neither give a deadly drug to anybody if asked for it, nor will I make a suggestion to this effect’, would result in the ‘doctor as healer’ becoming the ‘doctor as executioner’. In short, healing and euthanizing are simply not miscible and euthanasia can never be considered ‘medical treatment’.
Donald Boudreau was an Arnold P. Gold Foundation Associate Professor of Medicine when this manuscript was written and submitted. He is grateful for the financial support the foundation has provided in the past and requests that readers appreciate the opinions expressed herein are his personal views and not necessarily reflective of the perspectives of the Foundation, its staff, affiliates or benefactors.
Google Scholar
Google Preview
- suicide, assisted
- medical management
Email alerts
Citing articles via.
- Recommend to your Library
Affiliations
- Online ISSN 1471-8391
- Print ISSN 0007-1420
- Copyright © 2024 Oxford University Press
- About Oxford Academic
- Publish journals with us
- University press partners
- What we publish
- New features
- Open access
- Institutional account management
- Rights and permissions
- Get help with access
- Accessibility
- Advertising
- Media enquiries
- Oxford University Press
- Oxford Languages
- University of Oxford
Oxford University Press is a department of the University of Oxford. It furthers the University's objective of excellence in research, scholarship, and education by publishing worldwide
- Copyright © 2024 Oxford University Press
- Cookie settings
- Cookie policy
- Privacy policy
- Legal notice
This Feature Is Available To Subscribers Only
Sign In or Create an Account
This PDF is available to Subscribers Only
For full access to this pdf, sign in to an existing account, or purchase an annual subscription.
- Help & FAQ
Voluntary euthanasia: A utilitarian perspective
- Center for Human Values
Research output : Contribution to journal › Article › peer-review
Belgium legalised voluntary euthanasia in 2002, thus ending the long isolation of the Netherlands as the only country in which doctors could openly give lethal injections to patients who have requested help in dying. Meanwhile in Oregon, in the United States, doctors may prescribe drugs for terminally ill patients, who can use them to end their life - if they are able to swallow and digest them. But despite President Bush's oft-repeated statements that his philosophy is to 'trust individuals to make the right decisions' and his opposition to 'distant bureaucracies', his administration is doing its best to prevent Oregonians acting in accordance with a law that its voters have twice ratified. The situation regarding voluntary euthanasia around the world is therefore very much in flux. This essay reviews ethical arguments regarding voluntary euthanasia and physician-assisted suicide from a utilitarian perspective. I shall begin by asking why it is normally wrong to kill an innocent person, and whether these reasons apply to aiding a person who, when rational and competent, asks to be killed or given the means to commit suicide. Then I shall consider more specific utilitarian arguments for and against permitting voluntary euthanasia.
All Science Journal Classification (ASJC) codes
- Health(social science)
- Health Policy
Access to Document
- 10.1111/1467-8519.00366
Other files and links
- Link to publication in Scopus
- Link to the citations in Scopus
Fingerprint
- Euthanasia, Active, Voluntary Medicine & Life Sciences 100%
- Euthanasia Arts & Humanities 90%
- euthanasia Social Sciences 66%
- Doctors Arts & Humanities 26%
- Capital Punishment Medicine & Life Sciences 22%
- Ethical Review Medicine & Life Sciences 20%
- Assisted Suicide Medicine & Life Sciences 19%
- George W. Bush Arts & Humanities 18%
T1 - Voluntary euthanasia
T2 - A utilitarian perspective
AU - Singer, Peter
PY - 2003/10
Y1 - 2003/10
N2 - Belgium legalised voluntary euthanasia in 2002, thus ending the long isolation of the Netherlands as the only country in which doctors could openly give lethal injections to patients who have requested help in dying. Meanwhile in Oregon, in the United States, doctors may prescribe drugs for terminally ill patients, who can use them to end their life - if they are able to swallow and digest them. But despite President Bush's oft-repeated statements that his philosophy is to 'trust individuals to make the right decisions' and his opposition to 'distant bureaucracies', his administration is doing its best to prevent Oregonians acting in accordance with a law that its voters have twice ratified. The situation regarding voluntary euthanasia around the world is therefore very much in flux. This essay reviews ethical arguments regarding voluntary euthanasia and physician-assisted suicide from a utilitarian perspective. I shall begin by asking why it is normally wrong to kill an innocent person, and whether these reasons apply to aiding a person who, when rational and competent, asks to be killed or given the means to commit suicide. Then I shall consider more specific utilitarian arguments for and against permitting voluntary euthanasia.
AB - Belgium legalised voluntary euthanasia in 2002, thus ending the long isolation of the Netherlands as the only country in which doctors could openly give lethal injections to patients who have requested help in dying. Meanwhile in Oregon, in the United States, doctors may prescribe drugs for terminally ill patients, who can use them to end their life - if they are able to swallow and digest them. But despite President Bush's oft-repeated statements that his philosophy is to 'trust individuals to make the right decisions' and his opposition to 'distant bureaucracies', his administration is doing its best to prevent Oregonians acting in accordance with a law that its voters have twice ratified. The situation regarding voluntary euthanasia around the world is therefore very much in flux. This essay reviews ethical arguments regarding voluntary euthanasia and physician-assisted suicide from a utilitarian perspective. I shall begin by asking why it is normally wrong to kill an innocent person, and whether these reasons apply to aiding a person who, when rational and competent, asks to be killed or given the means to commit suicide. Then I shall consider more specific utilitarian arguments for and against permitting voluntary euthanasia.
UR - http://www.scopus.com/inward/record.url?scp=0142147067&partnerID=8YFLogxK
UR - http://www.scopus.com/inward/citedby.url?scp=0142147067&partnerID=8YFLogxK
U2 - 10.1111/1467-8519.00366
DO - 10.1111/1467-8519.00366
M3 - Article
C2 - 14959723
AN - SCOPUS:0142147067
SN - 0269-9702
JO - Bioethics
JF - Bioethics
158 Euthanasia Topics & Essay Examples
If you’re writing a euthanasia essay, questions and topics on the subject can be tricky to find. Not with our list!
- 📑 Aspects to Cover in a Euthanasia Essay
🏆 Best Euthanasia Essay Examples & Topics
💡 clever euthanasia titles, 🎓 simple & easy euthanasia essay titles, ✅ most interesting euthanasia topics to write about, ❓ euthanasia essay questions.
Our experts have prepared a variety of ideas for your paper or speech. In the article below, find original euthanasia research questions and essay titles. And good luck with your assignment!
📑 Aspects to Cover in an Euthanasia Essay
Euthanasia is the process of intentional life ending. Its goal is to stop patients’ suffering and pain. In today’s world, euthanasia is a debatable topic, and there are many questions about it.
Euthanasia essays can help students to raise awareness of the process and its aspects. That is why it is crucial to research this issue and write papers on it.
You can discuss various problems in your essay on euthanasia, as there is a broad variety of related issues. You can choose the one you are the most concerned about, search for euthanasia essay questions online or consult your professor.
Here are some examples of euthanasia essay topics and titles we can suggest:
- The benefits and disadvantages of a physician-assisted suicide
- Ethical dilemmas associated with euthanasia
- An individual’s right to die
- Euthanasia as one of the most debatable topics in today’s society
- The ethical dilemma around euthanasia
- The ethics associated with voluntary euthanasia
- Can euthanasia be considered murder?
- Euthanasia debate: Should the government legalize this procedure?
- The legality of physician-assisted suicide in today’s society
Once you have selected one of the euthanasia essay titles, you can start working on your paper. Here are some important aspects to cover:
Start from developing a solid euthanasia essay thesis. You should state the main idea of your paper and your primary argument clearly. A thesis statement can look like this: Euthanasia is beneficial for patients because it prevents them from suffering. Euthanasia can be equal to murder.
- Remember to include a definition of euthanasia and related terms, such as physician-assisted suicide. Your audience should understand what you are talking about in the essay.
- Do not forget to include the existing evidence on the issue. For instance, you can research euthanasia in different countries, the debates around its legalization, and all other aspects related to the problem. Support your claims with facts and cite your sources correctly.
- Legal and ethical questions are some of the most significant aspects you should cover in the essay. Discuss the potential benefits and disadvantages of the procedure, as well as its impact on patients’ families and medical professionals.
- If you are writing an opinion paper, do not forget to state your opinion clearly. Include relevant experience, if possible (for example, if you work at a hospital and patients have asked you about the procedure). Have you met people who could have benefited from euthanasia? Include their stories, if applicable.
- Do not forget to cover the legal aspects of euthanasia in your state. Is it legal to perform some form of euthanasia where you live or work? Do you think it is beneficial for the patients?
- Remember to look at the grading rubric to see what other aspects you should cover in your paper. For example, your professor may want you to state a counter-argument and include a refutation paragraph. Make sure that you follow all of your instructor’s requirements.
- If you are not sure that you have covered all the necessary questions related to your issue, check out related articles and analyze the authors’ arguments. Avoid copying other people’s work and only use it as an inspiration.
Please find our free samples below with the best ideas for your work!
- Euthanasia: Advantages and Disadvantages The most heavily criticized of all such similar actions is involuntary euthanasia which bears the brunt of all severe protests against the issue, with involuntary euthanasia being dubbed as the deprivation of an individual of […]
- Arguments in Favor of Euthanasia Due to the sensitivity of the issue, laws that will protect the rights of both the patient and the physicians who practice euthanasia should be put in place.
- Consequentialism: Euthanasia and Physician-Assisted Suicide People against euthanasia view the consequences of legalization as a gateway to other unethical practices being accepted, which is a slippery slope that could lead to adverse consequences to the fundamental principles and values of […]
- The Morality of Euthanasia In the meantime the medication and the doctors are not trivial anymore in stopping the pain and the victim despite all the sufferings, he or she is in a vegetative state and there is nothing […]
- Euthanasia as Self-Termination Velleman believes that a person should not have the right to end their life as it can make other people suffer, but there is an objection to his opinion related to that person’s own pain.
- David Velleman’s Views on Euthanasia Velleman is correct in his conviction that in this case, the patient’s decision will be the outcome of a federal right to die; the situation with euthanasia is common to that of abortion with the […]
- Why Active Euthanasia is Morally Wrong The issue of active euthanasia has come to the attention of the public over the past decades as more people demand for the right to be assisted to die.
- Advantages and Disadvantages of Euthanasia in Modern Society In its turn, this points out to the fact that, in the field of health care, the notion of medicinal compassion organically derives out of the notion of scientific progress, and not out of the […]
- Euthanasia in Christian Spirituality and Ethics By examining Christian’s views on the fallenness of the world, the hope of resurrection, and the value of a person’s life, one can see that euthanasia is not a morally acceptable option for a Christian […]
- An Argument Against Euthanasia 5 Generally, it is contrary to the duty of the subject of euthanasia and that of those who intend to perform the mercy killing to take one’s life based on their own assessment of the […]
- The Problem of Euthanasia in Animal Shelters Animal shelters are forced to euthanize animals for a number of reasons which includes: Lack of funds to treat sick animals, overcrowding as a result of the increased number of animals brought in by owners […]
- Euthanasia: Legalisation of a Mercy Killing The fact that the minority of countries and only several states in the US accept euthanasia proves that today people are still not ready to accept it as a mercy.
- Euthanasia and Assisted Suicide The final act that results in the death of the person is however usually performed by the person intending to die after the provision of information, advice and even the ways through which he or […]
- The Death Definition and the Need for Euthanasia If the concept of the soul is to be believed in, then one’s death is simply a process that detaches the soul from the body.
- Euthanasia as a Polarizing Issue The example of a plethora of countries shows that the inclusion of assisted suicide is not detrimental to the broad society.
- Rachel’s Stance on Euthanasia: Passive and Active Killing Despite the appealing nature of Rachel’s argument, his claims of equity of killing and letting a person die are not ethically right. A major distinction between killing and witnessing death is the level of responsibility […]
- Euthanasia for Terminally Ill People: Pros & Cons Despite the fact that euthanasia causes a lot of controversy, every person should have the right to end suffering. Permission of euthanasia is the realization of a person’s right to dispose of their body.
- Euthanasia: Arguments for and Against If the disease has reduced a person to a vegetative state and deprived them of consciousness, then their life is no longer fully human and therefore is not considered a blessing.
- Analysis of Ethical Dilemma: Euthanasia One of these is the right to live, which includes much more than the ability to simply exist, and suggests an adherence to a minimum of quality and self-determination.
- Euthanasia-Related Ethical and Legal Issues There are no discussions about whether the person has the right to commit suicide or not because most individuals agree that it is the decision of the adult person who can dispose of their life.
- Euthanasia: Legal Prohibitions and Permits In addition, it is necessary to take into account the right of a suffering person to get rid of the suffering of loved ones.
- Euthanasia: Why Is It Such a Big Problem? Thus, according to the utilitarian viewpoint, there is no problem with euthanasia as along as it is better for the patient. Who is it to decide what is better for the patient?
- Euthanasia and Assisted Suicide as a Current Issue in Nursing Nowadays, even in nations where the procedure of euthanasia and assisted suicide has been legal for decades, this topic continues to be controversial due to ethical and policy issues. However, in the light of the […]
- Euthanasia and Its Main Advantages However, after realizing the condition is untreatable and having the consent of both the sick person and the relatives, undertaking assisted suicide will enable the patient to evade extreme suffering.
- Euthanasia: Nurses’ Attitudes Towards Death The weakest part of the article is that most of the participants did not clearly define the concept of euthanasia, which casts doubt on the reliability of the sampled data.
- Right to Die With Euthanasia Methods The possible answer is to develop the functionality of both ordinary public hospitals and hospices that are located in their departments. In addition, it is critical to specify the desirable methods of euthanasia.
- “Active and Passive Euthanasia” by James Rachels The second issue about euthanasia that Rachels raises is the difference between killing and allowing one to die. For Rachels, it is necessary to emphasize that killing is sometimes even more humane than allowing one […]
- Arguments Against Legalization of Euthanasia Although the PAS/E should be offered voluntarily to a patient, in some cases it is offered in secret by physicians to patients who are perceived to be dying.
- Euthanasia: The Terri Schiavo Case Analysis The long-term judicial resolution of the Terri Schiavo case was related to the bioethical problem of the humanity of euthanasia, which had many opponents and supporters.
- Can Euthanasia Be Considered Ethical Consequently, from this perspective, the act of euthanasia would be regarded as violence to someone else’s life. As a result, euthanasia is likely to be considered unethical from the point of view of any of […]
- “Active and Passive Euthanasia” and “Sexual Morality” According to Scruton, morality is a constraint upon reasons for action and a normal consequence of the possession of a first-person perspective. For Scruton, sexual morality includes the condemnation of lust and perversion that is, […]
- Nursing Role in Euthanasia Decision and Procedures The weakest point is the lack of analysis of other factors’ influence on the process of euthanasia. The researchers discovered that the role of nurses in euthanasia is underestimated.
- Aspects of Nursing and Euthanasia The subject of the research by Monteverde was to ask people who work in the medical sphere and face the necessity for euthanasia, whether they are for or against it, and why.
- Pros and Cons of Euthanasia from an Ethical Perspective Primarily, this is apparent on American soil, in which some states decriminalized euthanasia, although the supreme court maintained that there is no law that legalized the practice nor the ban of the mentioned act.
- Euthanasia in the Context of Christianity The questions addressed in the paper include the notions of fall and resurrection as means of interpreting suffering, the Christian stance on the value of human life and euthanasia, and the discussion of possible solutions […]
- Nursing Practice and Euthanasia’s Ethical Issues Effective healthcare management is the involvement of all stakeholders, such as CMS, and the federal government in the decision-making process to improve the sustainable growth in the effectiveness of Medicaid.
- Counseling on Euthanasia and End-of-Life Decision The immediate dynamic killing is a clinical demonstration coordinated to the hardship of life, while a doctor helped self-destruction is a demonstration of the doctor where he gives the patient a medicament for taking life.
- Euthanasia and Physician-Assisted Suicide Articles According to the methods of application, there are two main types of euthanasia: “active”, which consists in performing certain actions to accelerate the death of a hopelessly ill person, and “passive”, the meaning of which […]
- Legal and Ethical Issues of Euthanasia Davis argues that there exists a challenge on how to establish a consensus in the competing views regarding the desire for patients to have the choice to die with dignity while under pain and distress […]
- Debates on Euthanasia – Opposes the Use Therefore, the legal system should work hand in hand with healthcare shareholders in distinguishing the limits between the patients’ rights and the physicians’ accountability based on the possible life-limiting treatment choices.
- Active Euthanasia: Ethical Dilema In case of active euthanasia, it is the patient who requests the medical practitioner to end his or her life and the former abides by the wish.
- Euthanasia: Every For and Against Jane L Givens and Susan L Mitchell “Concerns about End-of-Life Care and Support for Euthanasia” Journal of Pain and Symptom Management Article in Press FOR The authors state socio-demographic characteristics of the people are the […]
- Pro Euthanasia in the United States The discussions of euthanasia implementation in the United States began in the early 19th century after the development of ether, which was applied to pain-relieving.
- Human Euthanasia Should Be Allowed It is stated that there is a shift in a social attitude towards human euthanasia, where people are beginning to realize that people’s lives are their rights.
- The Euthanasia in Humans The moral and ethical aspects of medical practice include not only the features of interaction with patients and other interested parties but also deeper nuances. In particular, one of the controversial and acute topics is euthanasia and its acceptability from different perspectives, including both patients’ and healthcare employees’ positions. In addition, religious issues are involved, […]
- Euthanasia: Philosophical Issues at Stake in Rodriguez I will argue that the prohibition of euthanasia contradicts utilitarianism and the principle of quality of life in particular, and can hardly be supported by paternalism since the ban does not benefit an individual’s life.
- “Euthanasia Reconsidered” by Deagle In more detail, there is a clearly discernible introduction that provides the background to the topic, introduces the thesis statement, and state the opinion of the author of the topic discussed.
- Euthanasia Movement in Modern America Euthanasia movements in modern America perfected the art of rhetoric in their communication and this worked for them in terms of winning the heart of the public.
- Euthanasia: The Issue of Medical Ethics In this respect, the position of a physician under the strain of extreme circumstances should be weighed about the value of compassion.
- The Dilemma of Euthanasia It is at this point, when it becomes a contention of professional ethics and moral considerations on the part of Jack and his wife on the one hand, and personal choice on the part of […]
- Euthanasia: Ethical Debates When a patient is in the final stage of life, sometimes, the disease or the conditions of the patient, cause a lot of physical and psychological suffering.
- Euthanasia Moral and Ethical Agitation If grandma were a dog, most all would agree that the only humane option would be to ‘put her to sleep.’ U.S.citizens are guaranteed certain rights but not the right to wouldie with dignity.’ This […]
- Life-Span Development: Terri Schiavo’s Euthanasia Case Euthanasia is the process of stopping the medical maintenance of a patient’s life when the patient/herself does not want to suffer anymore and the doctors are sure that no improvements in the patient’s condition are […]
- Euthanasia and Other Life Termination Options However, there is a strong case for helping terminally ill patients spend the remainder of their lives with care provided by the medical fraternity and with support from the state and insurance companies. And in […]
- The Problem of Euthanasia Nevertheless, we must recognize that the interruption of life, alone or with the help of doctors, is contrary to one of the basic tenets of Christianity: the more people suffer on earth, the easier it […]
- Euthanasia: Allow Them to Be Free From Body Euthanasia, the practice of deliberately bring about an easy, painless, and moderate death to a person who is in the last days of his life and can no more bear the pain of living, has […]
- Palliative Medicine Replacement for Euthanasia Euthanasia is not about helping ill and dying people to end their pain and bring comfort. Euthanasia undermines the core values of life and decreases the motivation to provide care for the dying.
- Euthanasia: A Legalized Right to Die Nothing could be further from the intent of those who favor a limited reconsideration of public policy in the areas of assisted suicide and voluntary active euthanasia.
- Euthanasia and Suicide Issues in Christian Ethics Based on the two perceptions of euthanasia, theological and professional, it is valid to say that assisted suicide is probably not the best way out.
- Euthanasia: Morals, Ethics, and the Value of Life James Rachels however disagrees with the position taken by doctors when it comes to active Euthanasia and argues that, given a case where the patient is in intolerable pain and is certain to die in […]
- Euthanasia. Arguments of Opponents The request of the patient to relieve them from Karma and sufferings that is clarification and healing, nobody gives the right to break life of a physical body.
- Attitudes Related to Euthanasia and Physician-Assisted Suicide Among Terminally Ill Patients Consequently, the outlined safeguard becomes the first line of defense in making sure that only the right individuals with chronic and incurable medical conditions benefit from assisted death.
- Active Euthanasia Legalization Controversy While many people present the notions of medical ethics, the right to life, and the availability of palliative care to oppose active euthanasia, there are those who support it since it is evidence-based in nature […]
- Dying With Dignity: Euthanasia Debate On the other hand, the supporters of the law claim that assisted death is not a suicide, and it allows more end-of-life options for terminally ill patients. The majority of people are concerned with control […]
- Euthanasia Legalization as an Unethical Practice The decision to legalize euthanasia is an idea that societies should ignore since it places many global citizens at risk, fails to provide adequate safeguards, diminishes social values, and undermines the teachings of Islam.
- The Ethics of Euthanasia In the analysis of the claims in favor and against euthanasia, the cause and effect relationships between the factors affecting the choice of euthanasia should be established.
- Today’s Moral Issues: Euthanasia To ensure that the right to life is respect, the law was amended to include assisted or aided suicide as a criminal offense.
- Controversial Issues of Euthanasia Decision We now had to make this difficult decision to end his life and relieve him of all the pain that he was undergoing.
- Confronting Physician-Assisted Suicide and Euthanasia It was because of that pain that led my mother and I to bring her to a Chinese holistic healer who treated her with some sort of secret Chinese medical injection.
- Assisted Suicide and Euthanasia Rights in Canada The article asserts that in the year 1993, Rodriquez petitioned in vain to the Supreme Court of Canada to allow her to undertake euthanasia. In the article, the author asserts that, in the year 1993, […]
- Euthanasia: “Being a Burden” by Martin Gunderson As it was implied in the Introduction, in his article, Gunderson argues in favor of the idea that it is utterly inappropriate to even consider the legalization of voluntary euthanasia, due to a number of […]
- Euthanasia: Fighting for the Right Cause Sommerville is a renowned Samuel Gale Professor of Law at the McGill University in Montreal, the Professor in the Faculty of Medicine, and the Founding Director of the Center for Medicine, Ethics, and Law. The […]
- Euthanasia as a Way of Painless Termination of Life The introduction of the Hippocratic School led to the abolishment of the practice. According to the approach, taking human life is unethical and violation of the core right to life.
- Euthanasia and Other Life-Destroying Procedures From this perspective, it is unethical to decide in favor of an end-of-life procedure on the condition that there are at least minimal chances for a patient’s survival.
- Ethics of Euthanasia and Pain-Relieving This leads to the historical argument that voluntary euthanasia is often the beginning of a slippery slope that gives rise to unintentional euthanasia and the murder of people who are unwanted in society.
- Euthanasia Legalization: Public Policy Debates The requirements of physicians to perform euthanasia and consideration of the second opinion eliminate the violation of legal and ethical stipulations, and thus, control the performance of euthanasia in health care environment. Opponents of euthanasia […]
- Euthanasia: Moral Rationalist View Human beings rely on the available evidence to generate beliefs about life and goals that should be attained, and thus the use of reason leads to success in these objectives.
- Euthanasia: Is It Worth the Fuss? In order to grasp the gist of the deliberations in this essay, it is important to first apprehend what the term euthanasia means and bring this meaning in the context of this essay.
- Active and Passive Euthanasia Analysis and Its Concept The issue of morality is one of the things that have to be mentioned when discussing the concept of euthanasia. In this instance, both the patient and the doctor know that there is no cure […]
- Euthanasia in Today’s Society Euthanasia is the deliberate termination of life with the intention of relieving a patient from pain and suffering. If the prognosis of a patient is gloomy, medical care providers may find it more compassionate to […]
- When Ethics and Euthanasia Conflict? The main aim is to reduce the lifetime of a patient who is terminally ill. There is a deep mistrust of the motivations that fuel euthanasia.
- Religions Views on Euthanasia This essay highlights religious thoughts with regard to the whole issue of euthanasia, bringing into focus the extent to which our society has been influenced by courtesy of the Dr.
- Euthanasia as the Key Controversy of the XXI Century The fact that in the present-day society, human life is put at the top of the entire list of values is a major achievement of the civilization and the fact that the current society is […]
- Euthanasia: Is It the Best Solution? In twentieth century, various agencies erupted to address the practice of euthanasia such as Voluntary Euthanasia Legislation Society in 1935, which was advocating for its legalization in London and the National Society for the Legalization […]
- Legalizing Euthanasia The are supporters of the idea that only God has the right to take human’s life, on the other hand, the sufferings of the person may be unbearable and they may ask for euthanasia to […]
- Euthanasia: Right to Live or Right to Die Euthanasia or mercy killing as it is informally referred is the act of ending a person life if it is deemed to be the only way to help a person get out of their suffering.
- A New Fight to Legalize Euthanasia Before settling down on the conclusion of the need to adopt the practice of euthanasia in our state, it is important to visit some basic aspects that are very key in the issue of euthanasia.
- The Ethics of Active Euthanasia In support of the euthanasia action, the argument is that there are circumstances when the rule of natural life can be violated.
- Is Euthanasia a Morally Wrong Choice for Terminal Patients? It is imperative to note that for both the opponents and proponents of euthanasia, the quality of life is usually the focal point, even though there is no agreement on the criteria of defining quality […]
- The Right to Life and Active Euthanasia The god of every individual should be the only one to bring death to a person and no person should have the authority to accept dying no matter the situation he/she is in.
- Singer’s Views on Voluntary Euthanasia, Non-voluntary Euthanasia, and Involuntary Euthanasia Hence, if a person consciously consents to die, there are no chances for recovery, and killing is the only way to deprive a patient from pain and suffering, euthanasia can be regarded as voluntary.
- Euthanasia Authorization Debate Euthanasia, which is equivalent to the termination of life, can be equated to a total breach of the principle of the sacredness of life, as well as the breach of the legal right of human […]
- Moral and Ethical Concerns of Euthanasia in Healthcare In the matter of euthanasia, professionals ought to decide between the overall good of the dying patient and that of other stakeholders.
- Good and Harm to Humanity of the Use a Euthanasia An Overview of Euthanasia The meaning of euthanasia has changed over the years from how it was originally construed to what it means to the contemporary world.
- Euthanasia and Meaning of Life The meaning of life is the most general aspect of judging about the requirements that must be set out by laws and people’s morals in regarding to the voluntary or involuntary taking of that life.
- Euthanasia: Your Right to Die? Although both positions can be supported with a lot of arguments, people should change their absolutely negative vision of euthanasia because the right to die with the help of physicians can be considered as one […]
- Euthanasia and Human’s Right to Die Trying to support human life with the help of modern equipment is a good idea, however, not in case there are no chances for a person to live without that equipment.
- Euthanasia Moral Permissibility Secondly, the application of voluntary euthanasia should not be regarded as the only way of reducing the pain that a patient can experience.
- Euthanasia (Mercy Killing) In some circumstances, the family and friends of the patient might request the hospital to terminate the life of the patient without necessarily informing the patient.
- Euthanasian Issues in Modern Society Is it possible to find the relief in the life which is full of pain and agony for those people who suffer from serious diseases and have only a little chance to get rid of […]
- Euthanasia From a Disciple of Jesus Christ in Today’s World Another form of euthanasia is that of Assisted Suicide where the person intending to end his/her life is provided with the necessary guidance, means as well as information as to how to go about the […]
- Euthanasia and Modern Society Towards this end Battin asserts that “the relief of pain of a patient is the least disputed and of the highest priority to the physician” in direct reference to sole and major reason of carrying […]
- Euthanasia: Moral Issues and Clinical Challenges Therefore, any law that rejects euthanasia is a bad one because it denies the patients the right and the liberty to die peacefully.
- Ethical Issues Surrounding the Choice of Euthanasia in the United States
- The Advantages and Disadvantages of the Legalization of Euthanasia
- Confronting Physician-Assisted Suicide and Euthanasia
- The Difference Between Active and Passive Euthanasia
- Euthanasia: Current Policy, Problems, and Solution
- The Permit and Legalization of Euthanasia for the Terminally Ill Patients
- Moral and Religious Differences Between Euthanasia and Suicide
- The Criticisms and Opposition of Euthanasia in Australia
- Assisted Suicide and Euthanasia It Is Not Murder, It Is Mercy
- The Factors That Influence the Legalization of Active and Passive Euthanasia in the United States
- Roman Catholic Church’s Teachings on Abortion and Euthanasia
- The Different Reasons Why People Are Against Euthanasia
- Religious and Ethical Arguments in Favour of Euthanasia
- The Moral and Ethical Views on the Goal of Euthanasia
- Euthanasia and the Role of Politics and Religion
- The Philosophical, Legal, and Medical Issues on Euthanasia
- General Information About Euthanasia and the Legality of Suicide in Australia
- The Nazi Euthanasia Programme Based on Racial Purity Theories
- Dr. Jack Kevorkian’s Role in Physician-Assisted Suicide and Euthanasia
- Utilitarian and Libertarian Views on Euthanasia
- The Moral and Religious Differences, if Any, Between Euthanasia and Suicide
- Biblical World View About the Euthanasia, Suicide, and Capital Punishment
- The Truth About Euthanasia and Assisted Suicide
- Tracing Back the Origins of the Practice of Euthanasia During the Greeks and Roman Times
- The Causes and Effects of Euthanasia and the Moral Right To Die
- The Arguments Against Euthanasia From a Standpoint of a Catholic Christian in the United States of America?
- Why Should Active Euthanasia and Physician-Assisted Suicide Be Legalized?
- What Are the Good and Bad Sides of Euthanasia?
- Do People Have To Commit Suicide by Euthanasia (Suicide by a Doctor)?
- What Is the Difference Between Passive and Active Euthanasia?
- What Are the Social Issues and Ethical Values of Euthanasia?
- What Is the Current Legal Situation Regarding Euthanasia?
- How Does Prohibition of Euthanasia Limit Our Rights?
- What Is the American Medical Association’s Attitude to Euthanasia?
- Can Hegelian Dialectics Justify Euthanasia?
- What Are the Viewpoints and Studies of the Legalization of Euthanasia in the United States?
- Why Does Parenting Make Euthanasia More Acceptable?
- What Are the Negative Arguments Against Euthanasia?
- Voluntary Euthanasia: What’s Right and Wrong?
- Why Can Christians not Accept Euthanasia?
- Can Euthanasia Help the Terminally Ill?
- What Are the Top Ten Reasons for Legalizing Euthanasia?
- Should Non Voluntary Euthanasia Be Legal?
- What Is the Difference Between Doctor-Assisted Suicide and Euthanasia?
- Why Should Euthanasia and Assisted Suicide Be Legalized?
- What’s Wrong With Involuntary Euthanasia?
- Why Are There So Different Views on Abortion and Euthanasia?
- How Would Christians Respond to the Issue of Abortion and Euthanasia?
- What Are the Objections To Legalizing Euthanasia in Hong Kong?
- How Does Euthanasia Devalue Human Life?
- What Are the Views and Arguments About Euthanasia?
- How May the Christian Faith Inform the Debate Over Euthanasia?
- What Does Euthanasia Mean to Society Today?
- What Are the Religious and Ethical Considerations to the Issue of Euthanasia?
- Euthanasia and Assisted Suicide – Who Wants It?
- Chicago (A-D)
- Chicago (N-B)
IvyPanda. (2024, February 28). 158 Euthanasia Topics & Essay Examples. https://ivypanda.com/essays/topic/euthanasia-essay-examples/
"158 Euthanasia Topics & Essay Examples." IvyPanda , 28 Feb. 2024, ivypanda.com/essays/topic/euthanasia-essay-examples/.
IvyPanda . (2024) '158 Euthanasia Topics & Essay Examples'. 28 February.
IvyPanda . 2024. "158 Euthanasia Topics & Essay Examples." February 28, 2024. https://ivypanda.com/essays/topic/euthanasia-essay-examples/.
1. IvyPanda . "158 Euthanasia Topics & Essay Examples." February 28, 2024. https://ivypanda.com/essays/topic/euthanasia-essay-examples/.
Bibliography
IvyPanda . "158 Euthanasia Topics & Essay Examples." February 28, 2024. https://ivypanda.com/essays/topic/euthanasia-essay-examples/.
- Human Rights Essay Ideas
- Suffering Essay Topics
- Morality Research Ideas
- Death Penalty Questions
- Healthcare Questions
- Suicide Topics
- Constitution Research Ideas
- Social Justice Essay Ideas
Why is the ethics of euthanasia wrong?
Affiliation.
- 1 Vytautas Magnus University, Gimnazijos g. 7, LT-3000 Kaunas, Lithuania.
- PMID: 16294446
Human beings are made in the image and likeness of God and are therefore of intrinsic worth or value, beyond all prices. Almost all Christian pro-life arguments spring from the fountain of personal dignity. Euthanasia would make moral sense only if it were possible to say, morally, that this dignity had vanished. To commit euthanasia is to act with the specific intention that somebody should be nobody. This is the fundamental error of all immorality in human relations. To commit euthanasia is to fail to see the intrinsic worth or dignity of the person. The judgement that what has worth, intrinsically, somehow does not have worth, is both logically and morally wrong. The ethics of euthanasia is based on dualistic anthropology and wrong moral presuppositions underlying the defence of euthanasia, namely, proportionalism and consequentialism. The basic claim of proponents of the ethics of euthanasia is that human persons are consciously experiencing subjects whose dignity consists of their ability to made choices and to determine their own lives. Bodily life, according to them, is a condition for personal life because without bodily life one cannot be a consciously experiencing subject. It means that bodily life is distinct from personal life. Thus, the body and bodily life are instrumental goods, goods for the person, not goods of the person. It thus follows that there can be such a thing as a life not worth living--one can judge that bodily life itself is useless or burdensome, and when it is, the person, i.e., the consciously experiencing subject, is at liberty to free himself of this useless burden. Today a key in fighting euthanasia and assisted suicide is better care for the sick and dying. The dignity of the sick cannot be erased by illness and suffering. Such procedures are not private decisions; they affect the whole society. Death with dignity, in the end, is the realisation that human beings are also spiritual beings. We have to promote the way of caring for the dying in which mercy is extended to the patients without inducing death.
- Christianity*
- Ethical Theory
- Euthanasia, Active / ethics*
- National Socialism
- Quality of Life
- Right to Die / ethics
- Value of Life*
- Wedge Argument

4 Non-Religious Reasons Why Euthanasia is Wrong
You are a member of the first generation of doctors in the history of medicine to turn their backs on the oath of Hippocrates and kill millions of old useless people, unborn children, born malformed children, for the good of mankind ― and to do so without a single murmur from the august New England Journal of Medicine . And do you know what you’re going to end up doing? You, a graduate of Harvard and a reader of the New York Times and a member of the Ford Foundation’s Program for the Third World? Do you know what is going to happen to you? You’re going to end up killing Jews. ― Walker Percy , The Thanatos Syndrome .
It is one thing to speak of the sanctity of life and of human life being created in the image and likeness of God . But what does one s ay when it comes to end-of life issues, and the question of euthanasia comes up? What does one do when a loved one is in immense suffering?

When people talk about whether euthanasia is right or wrong, two questions will inevitably come up:
- Why is euthanasia right (or wrong)?
- Should we not be able to determine the ultimate disposition of our own bodies?
Even from a non-religious standpoint, euthanasia is wrong for 4 reasons:
- Humans have great dignity.
- Voluntary euthanasia is a slippery slope.
- It puts pressure on “burdensome” individuals.
- It makes true palliative care worse.
We will review each of these reasons in detail.
Reason #1: Humans Have Greater Dignity
Some say that if one euthanizes their pets when they are old and suffering, the same should be true for humans. Some go so far as to say that, if humans are unable to choose euthanasia, their pets have more “rights” than they do.
The pain of watching a loved one suffer immensely, particularly in their final days, is indescribable. Understandably, we often wish to do anything to alleviate their suffering.
The fundamental problem with euthanasia is that it violates human dignity.
Human dignity doesn’t come from ability, wealth, mental state, or any other changeable factor. It comes directly from our humanity. This inherent and immutable dignity gives every human life value. Human dignity and the intrinsic value of human life are the bedrock of any sane structure of social ethics.
When we let anyone decide that a life is no longer valuable, even if it’s the individual making that decision, we are treating human dignity like a subjective opinion instead of an immutable reality. The attitude that human dignity is subjective is an essential ingredient to any kind of human rights abuse.
Even in a person’s final moments, even with immense suffering, everyone deserves to die a natural death. Humans have an intrinsic and unique value and worth, and hastening one’s death violates this worth.

In their final days, humans should opt for comfort care – or palliative care, as we will discuss below – while accepting a natural death. What is a “natural death?”
Natural death is when an individual allows their ailments to claim their life versus hastening their death or using physician-assisted suicide. By dying a natural death, one is not hastening their death through drugs or lack of food, for example. Instead, they are accepting their end as it comes naturally and living their final moments in the best comfort possible.
Reason #2: Voluntary Euthanasia is a Slippery Slope
Voluntary euthanasia is a slippery slope to involuntary euthanasia. Involuntary euthanasia involves killing a person when they either do not consent or are unable to consent (such as while in a coma).
If we allow individuals to choose physician-assisted suicide when they are suffering, what’s to stop the family of a patient from choosing euthanasia when their loved one is unconscious?

The Netherlands legalized euthanasia of newborns who are “defective,” which includes being “severely handicapped.” Killing newborns is not voluntary euthanasia. The newborn lacks the ability to consent.
Indeed, allowing voluntary euthanasia and expecting involuntary euthanasia to still be opposed is dangerous. Involuntary euthanasia can easily go under the radar , especially in the case of newborns and the elderly.
Many oppose the “slippery slope” argument, saying there is no evidence that allowing voluntary euthanasia would lead to involuntary euthanasia. They further argue that creating laws that draw a hard line between voluntary and involuntary euthanasia would prevent the slippery slope fear, that society can support the voluntary while strongly rejecting the involuntary.
However, allowing voluntary euthanasia and expecting involuntary euthanasia to be opposed in all cases is dangerous. A 2022 project concluded that legalized euthanasia presents too great a risk to vulnerable communities, namely, the disabled and terminally ill.
There’s also the concern that involuntary euthanasia will be used for those whose lives are not deemed “worth living,” such as deformed or disabled children, or for those with treatable conditions.

Canada is a Warning for Our Future
Canada’s “progressive” euthanasia and physician-assisted suicide laws are further down the slippery slope than our own. It can serve as a stark, real-life example of the slippery slope argument.
A Canadian veteran was offered euthanasia as the ideal solution when she couldn’t secure a stairlift for her home.
Another veteran was reportedly seeking treatment for PTSD injuries and had been improving when his VA counselor suggested physician-assisted suicide as the best option. What’s the point of having healthcare, if the go-to is euthanasia when someone is suffering?
Canada has expanded their euthanasia laws to include individuals with chronic conditions, even if those conditions are not life-threatening . But the expansion doesn’t stop there. There has been a push to legalize euthanasia for individuals suffering solely from a mental illness, such as depression. This expansion was set to take place in March 2023, but they extended the date to March 2024.
What the future may reap with such policies is bleak. Canada has government-funded healthcare. If euthanasia becomes the norm for illnesses and conditions, will the government stop funding many sectors in healthcare, with the assumption that individuals will choose euthanasia?

A Forbes article addresses concerns felt by doctors:
“Dr. Ramona Coelho, a Canadian family physician told the Associated Press, ‘The whole premise of the legislation is built on a discriminatory approach to people with disabilities. … Most Canadians think that this is a service of compassion offered for people who have nothing left to be offered and are being offered death as a way out. When, in fact, the system is being applied so liberally and so easily in such a short time period that people are dying who would’ve recovered with greater care and resources to live.’ It is a view echoed by Marie-Claude Landry head of the country’s human rights commission who said that euthanasia ‘cannot be a default for Canada to fulfill its human rights obligations.’ Addressing the notion that, when patients are presented with treatment options by doctors, they are likely to be viewing their future life with disability through the lens of economic deprivation, Landry said, “In an era where we recognize the right to die with dignity, we must do more to guarantee the right to live with dignity.”

Related: Is Euthanasia Ever Justified?
Reason #3: Allowing Euthanasia Puts Pressure on “Burdensome” Individuals
Related to Reason #2, if euthanasia is allowed, it indicates that there are individuals in society who we are unwilling to help and care for. Society should be sensitive and caring to those who have more challenges.
Normalized and encouraged euthanasia further puts pressure on these individuals to take their own lives to make life “easier” for the society who spurns them. Such individuals would include disabled, elderly, mentally challenged, or even those who suffer from mental illnesses such as anxiety or depression (such as we are seeing in Canada).
Professor Theo Boer is a leading expert in the ethics of euthanasia. He is a member of a review committee that receives information regarding every euthanasia case in the Netherlands. He expressed concern regarding the pressure that normalized euthanasia puts on “burdensome” individuals.
Further, a poll by the disability charity Scope found that 64% of disabled respondents would be concerned with a relaxation of the laws surrounding assisted suicide. They fear that, by having broader assisted suicide services, disabled individuals will be pressured to choose this option.

An article on The Guardian on how disabled individuals are pressured to choose assisted suicide:
“Some 5% of people in Oregon dying by assisted suicide cited financial pressures as a cause. Meanwhile, the number citing being a ‘burden on family/friends/caregivers’ increased from 13% in 1998 to 55% in 2017 . This tallies with Scope’s research that the majority of people with disabilities are concerned that legalising assisted suicide might lead to disabled people choosing it in order not to be a burden on others. Under austerity people who are disabled, ill or elderly are constantly taught that funding our health and social care is a burden – that we are inherently a burden.”
Society should never shrug off the responsibility of taking ca re of its members, particularly those who need it the most. There is no limit to how far the ugly arms of euthanasia could reach. But these individuals are loved and valued human beings with intrinsic worth. They should receive the same respect, honor, and kindness as the rest of society.
Indeed, those who choose euthanasia may well be choosing it out of a fear of being “burdensome” to their loved ones. Instead, th ese individuals should be reassured that their lives are worth living and that they have dignity. They are worthy of care, support, comfort, and compassion in their final days. Palliative care is a worthy alternative to euthanasia. It honors the patient’s dignity and gives them comfort as they prepare for their final day.

Which brings us to the final reason euthanasia is wrong.
Reason #4: Allowing Euthanasia Makes True Palliative Care Worse
Euthanasia is, by its nature and definition, in complete opposi tion to the principle of “do no harm.” Thus, euthanasia and palliative care are completely incompatible . Palliative care seeks to provide dignity, comfort, and compassion in a person’s final days. It seeks to minimize or eliminate pain and to give comfort to the patient. Palliative care is thus in perfect accord with the m edical principle of “do no harm.” Not only does it make euthanasia obsolete, but it also makes it unthinkable.
It also can be said that palliative care affords an understanding of one’s own worthiness and dignity, even in the midst of suffering. A 2018 study found that 86% of patients who received palliative care did not request euthanasia. Euthanasia, meanwhile, is the ultimate despair, the la st-ditch effort to make things “easier” for the patient’s family and loved ones. In reality, a family should know their own individual dignity and worth and honor themselves and their family members.

If euthanasia is pushed and normalized, palliative car e is impossible. Having euthanasia as the norm makes it expected, so palliative care becomes unexpected and neglected. Those who do not choose euthanasia may be seen as a burden on the healthcare system. Those who do not have access to needed care may also be pushed towards euthanasia, as seen in Canada with the two veterans. Indeed, we’ve seen assisted suicide suggested for fin ancial reasons .
Dr. Madeline Li, a Canadian psychiatrist who’s helped hundreds of patients with physician-assisted suicide, expressed concern over where Canada is heading with its euthanasia expansions: “Making death too ready a solution disadvantages the most vulnerable people, and actually lets society off the hook. I don’t think death should be society’s solutions for its own failures.”
In countries where the government funds healthcare (thus providing universal healthcare), normalized and pushed euthanasia would encourage the government to limit or even halt funding of end-of-life healthcare beyond euthanasia. In other words, in such countries, the government does not have an interest in paying for palliative services, assuming or wanting the patient to choose euthanasia as the cheaper option.

Allowing and normalizing euthanasia takes away from the dignity and worth that palliative care encourages and emphasizes.
Final Thoughts
Humans deserve more than hastening their death in the painful final days. Instead of euthanasia, we should be pushing for improved palliative care to give comfort to individuals in their final days in accordance with their worth and dignity.
This article was originally published in July 2020 by Dr. Brian Clowes and was most recently updated in June 2023 by Marisa Cantu.
Share on Facebook Share on X (Twitter) Share on Email Share on SMS
Related Content

Physician-Assisted Suicide for Terminally Ill Patients

Is Euthanasia a Slippery Slope?

6 Types of Euthanasia: Is It Ever Justified?

Human Suffering Does Have a Purpose

Church Teachings on Euthanasia

The Fractured History of the Hemlock Society

Is Nazi Euthanasia Resurfacing in the U.S.?

The Hippocratic Oath: A Pledge to Respect Life

25 Bible Verses and the Problem of Euthanasia

Catholic Bioethics and the Moral Treatment of Human Beings

Brian Clowes, PhD
Dr. Brian Clowes has been HLI’s director of research since 1995 and is one of the most accomplished and respected intellectuals in the international pro-life movement. Best known as author of the most exhaustive pro-life informational resource volume The Facts of Life , and for his Pro-Life Basic Training Course , Brian is the author of nine books and over 500 scholarly and popular articles, and has traveled to 70 countries on six continents as a pro-life speaker, educator and trainer.

Marisa Cantu
Marisa Cantu has an MS in political science and international affairs with a BA in political science and has also studied international studies and French. She has a strong background in nonprofit work, research, writing, and policy proposal and analysis.
In her free time, Marisa enjoys painting, writing, cooking, spending time with her husband and playing with her dog.

Everything you said sounds extremely biased. Not everyone is religious, and as an athiest, I can easily make several of these arguments; I totally agree that under absolutely NO circumstances, should euthanasia be actively encouraged; let alone should it ever be used on a non-consenting human.
I have the same belief for humans as I do for animals: No creature should be forced to surrender their lives, or their organs or anything else, for others “convenience”.
However, I can see where your argument falls apart at the seams: you repeatedly, and emphatically, turn into a “strawman”, as well as a “slippery slope”, and you overemphasize every single time your argument is “proven”, while willfully ignoring anything that could be used as evidence against this.
If laws were put in place to protect all minors, and laws put in place that those seeking euthanasia for non-lethal reasons (including poverty and mental illness) would automatically have to go through various programs that would give their lives dignity (one point I agree with wholeheartedly); and that no matter what, every person would be granted the right to live, and the right to all needed healthcare free of charge; thus protectong all other forms of healthcare, including pallative care (which could, ideally, coexist with patient requested euthanasia, in extremely painful circumstamces); And if we were to simply apply similar to pets as well (pets may receive pallative care, we stop euthanizing healthy individuals no matter the reason, etc); Then we could have a much more friendly, bearable world, that is still quite safe for the living, without being a trap of torture.

The issue I have with your opinion piece is that it is quite intentionally selective in the examples used. They are of the “Supposed brain-dead comatose patient surprises evil doctors and gets up to pick up a puppy” variety.
I’m literally in the middle of experiencing a quite different situation. I am the caregiver for a great friend I’ll call Fred. Fred is an 80-year-old Marine…the “tough as nails” type who never showed a moment of physical pain. He also smoked for over 60 years. He knew that his hacking cough probably meant a bad outcome, so he ignored it for years.
When his body started aching to the point of unbearable pain, he finally agreed to let me take him for a visit to the doctor. It’s now six weeks later. Stage 4 lung cancer, with the pain being caused by the cancer spreading to his bones. I watched as the radiologist showed the CT and PET scans, along with Fred. The technology is amazing. The results were close to horrifying. The computer display took a path that started at Fred’s jawline, and travelled to knee level. The radiologist would pause at each of the affected bones. By “affected”, I mean each area with a mass that was actively eating away at his bones. Fred’s right shoulder blade was missing one-third of it’s bone. The same with both pelvic bones, a few ribs, and quite a few more bones. He had a fracture in his right mid-humerus. The doctor said that, given the fragility of his bones, the fracture could easily have been caused by a sneeze.
Fred is going to die today, tomorrow, likely no more than three days from now. He’s not going to miraculously rise up and pick up a granddaughter or a puppy. I’ll tell you what he IS going to do, and what he’s been doing for five days now: He is going to agonize in a state of semiconciousness while breakthrough pain causes his body to twitch uncontrollably. This tough-as-nails Marine screams every two or three minutes….a long, desperate scream that even makes his nurses cringe. How do I know this? Because I’ve spent hours at his bedside, his hand in mine, praying silently that his body finally succumbs. I wonder how many of the commenters to this article, who opine so stridently and with such conviction, even sat and watched a loved one suffer so brutally.
And the “But in this day and age, with modern pain medications, no one needs to suffer before dying” contention? I speak from first hand observation: It was bull**** 20 years ago when my mother died a very painful cancer death, and it remains so today. Why? Because when you see your loved one in agony, and try to have the pain meds increased, the response is today what it was 20 years ago: “If we give him any more medication, we run the risk of stopping his heart. We aren’t allowed to do that.” And to give you an idea of just how effective those end-of-life drugs are: Fred is receiving a strong dose of morphine EVERY HOUR, along with a daily fentenyl patch. Two of the strongest medications available. His screams of agony as he lies in a fetal position shows just how effective they are. There’s a reason it’s called “breakthrough pain”.
So forgive me if I find your article disingenuous at best, and intentionally misleading at worst. You cite examples of people in comas, while intentionally overlooking that there are some patients who will NOT rise up miraculously. The discussion is one of great nuance, but you paint with a broad brush. I suspect that your mind won’t be changed unless and until you have to hold that loved one’s hand and watch him in agony. You might then realize that your claims that the moment of a person’s death should be “God’s will” ring hollow. To subscribe such mercilessness on God is sacrilegious in and of itself. I also suspect that you will delete this post, as it doesn’t fit easily into your simplistic rationale.
One last thing: I pray that you never suffer as Fred suffers at this moment, and I pray that you never see what I’ve seen.
Peter, We are so very sorry for Fred’s suffering. It is no easy thing to accompany a loved one in his final days, even less so when great suffering is involved. Our sympathy goes out to you both and to all who are dear to Fred and will feel his loss. Fred’s life, and indeed all human life, is a gift from God. I humbly offer my prayers and the following resource to better explain the redemptive power of suffering: https://www.hli.org/resources/slippery-slope-euthanasia/

Peter: 1) I’m so very sorry that you’ve had to endure watching a loved one leave this world like that. While I do not 100% know your pain, I empathize with you very deeply… my mother passed away in 2020 while I was in bootcamp from Stage 4 uterine cancer that, by the time it was discovered, had spread to most of her body. This was about a few years after a very successful surgery that removed a malignant glioblastoma in her brain. 2) I’m very glad you decided to post your comment (and that it remained up), as I found this article left an exceedingly bad taste in my mouth, as well. As you cited, the medical examples used are extremely narrow and all follow one “genre.” I actually couldn’t believe what I was reading, and I could not finish the article, as such. 3) I hope you have the love and support that YOU need after going through such an ordeal with your dear friend.

I would like a printable copy of your this article to share with the Drs who are trying to euthanize my father. We’re fighting for his life and trying to to get him to a safe place out of secular hospitals. We have a very short window to do so. We need to find a pro-life neurologist in CA and a compassionate healthcare facility willing to take him and rescue a living person from the tyranny of wanna-be-god doctors and empowered by corrupt laws.
Thanks for your interest. When viewing this article on the HLI website, you should see a “bar” of icons: Facebook, Instagram, Twitter, etc., and a Printer Friendly icon. Clicking that printer icon will allow you to print the article in PDF format.

I have got so many facts from this article to my debate “Euthanasia should be banned”. Thank you so much !!!

God bless you. Every life soul matters.

Dear Mr. Clowes,
I enjoyed your article. Well written. Thanks.
Derek Simpson
Leave a Comment Cancel Reply

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Ann Med Surg (Lond)
- v.75; 2022 Mar
Euthanasia and assisted suicide: An in-depth review of relevant historical aspects
Yelson alejandro picón-jaimes.
a Medical and Surgical Research Center, Future Surgeons Chapter, Colombian Surgery Association, Bogotá, Colombia
Ivan David Lozada-Martinez
b Grupo Prometheus y Biomedicina Aplicada a las Ciencias Clínicas, School of Medicine, Universidad de Cartagena, Cartagena, Colombia
Javier Esteban Orozco-Chinome
c Department of Medicine, RedSalud, Santiago de Chile, Chile
Lina María Montaña-Gómez
d Department of Medicine, Keralty Salud, Bogotá, Colombia
María Paz Bolaño-Romero
Luis rafael moscote-salazar.
e Colombian Clinical Research Group in Neurocritical Care, Latin American Council of Neurocritical Care, Bogotá, Colombia
Tariq Janjua
f Department of Intensive Care, Regions Hospital, Minnesota, USA
Sabrina Rahman
g Independent University, Dhaka, Bangladesh
End-of-life care is an increasingly relevant topic due to advances in biomedical research and the establishment of new disciplines in evidence-based medicine and bioethics. Euthanasia and assisted suicide are two terms widely discussed in medicine, which cause displeasure on many occasions and cause relief on others. The evolution of these terms and the events associated with their study have allowed the evaluation of cases that have established useful definitions for the legal regulation of palliative care and public policies in the different health systems. However, there are still many aspects to be elucidated and defined. Based on the above, this review aimed to compile relevant historical aspects on the evolution of euthanasia and assisted suicide, which will allow understanding the use and research of these terms.
- • The history of euthanasia and assisted suicide has been traumatic.
- • The church and research have been decisive in the definition of euthanasia.
- • The legal framework on the use of euthanasia and assisted suicide has been strengthened.
1. Introduction
Euthanasia and assisted suicide are two topics discussed throughout history, mainly because they fall within the scope of life as a human right, which has been universally defended for many years [ 1 ]. However, the mean of the word euthanasia as good death generates conflicts at social, moral, and ethical levels. Mainly because death is a loss, it is difficult to understand it as something positive and; additionally, several historical events such as the Nazi experiments related the term euthanasia more to murder than to a kind and compassionate act [ 1 ]. More current texts mention that euthanasia is the process in which, through the use or abstention of clinical measures, the death of a patient in an incurable or terminal condition can be hastened to avoid excessive suffering [ 2 ].
The difference between euthanasia and assisted suicide is that in the latter, the patient takes the final action; however, both practices can be combined in the term assisted death [ 2 ]. At present, several countries authorize assisted death, including Holland, Luxembourg, and Canada [ 3 ]. Belgium and Colombia have regulations that decriminalize only euthanasia; other places where assisted suicide is legal are Switzerland and five states of the United America states, specifically Oregon, Vermont, Washington, California, and Montana [ 2 , 3 ]. Spain recently joined the list of countries that have legislated on euthanasia through the organic law March 2021 of March 24 that regulates euthanasia in that state in both public and private institutions [ 4 ]. The fact that more and more countries were joining the legislation on euthanasia and assisted suicide has brought to light the opinion of thinkers, politicians, philosophers, and physicians. Several nations have initiated discussions on the matter in their governmental systems. Latin America is trying to advance powerfully in this medical-philosophical field. Currently, in Chile, the “Muerte digna y cuidados paliativos” law, which seeks to regulate the issue of euthanasia and assisted suicide in the country, is being debated in Congress [ 5 ].
It is essential to know the point of view of physicians on euthanasia and assisted suicide, especially taking into account that these professionals who provide care and accompany patients during this moment, which, if approved, would involve the medical community in both public and private health systems. Although it seems easy to think that physicians have a position in favor of the act of euthanasia because they are in direct and continuous contact with end-of-life situations, such as palliative care, terminally ill, and critically ill patients. It is important to remember that the Hippocratic medical oaths taken at the time of graduation of professionals are mostly categorical in mentioning the rejection of euthanasia and assisted suicide [ 6 ]. Furthermore, it is also important to note that many of the oldest universities in the Western world originated through the Catholic Church; and just this creed condemns the practice of euthanasia and continues to condemn it to this day. This situation generates that many medical students in these schools have behaviors based on humanist principles under the protection of faith and religion and therefore reject the possibility of euthanasia [ 7 , 8 ].
The relevance of the topic and the extensive discussion that it has had in recent months due to the COVID-19 pandemic added to the particular interest of bioethics in this topic and the need to know the point of view of doctors and other health professionals on euthanasia and assisted suicide.
2. Origin and meaning of the term euthanasia
The word euthanasia derives from the Greek word “eu” which means good, and the word “thanatos” which means death; therefore, the etymological meaning of this word is “good death”. Over time the evolution of the meaning has varied; even as we will see below was considered a form of eradication of people categorized under the designation of leading a less dignified life. Assisted suicide is a condition in which the patient is the one who carries out the action that ends his life through the ingestion of a lethal drug but has been dispensed in the context of health care and therefore called assisted. This care is provided by a physician trained in the area. However, it requires the prior coordination of a multidisciplinary team and even the assessment by an ethics committee to determine that the patient is exercising full autonomy, free from coercion by the situation he/she is living and free from the fatalistic desires of a psychiatric illness [ 9 ]. In a more literary sense, the word euthanasia meaning of “giving death to a person who freely requests it in order to free himself from suffering that is irreversible and that the person himself considers intolerable” [ 9 ].
Some authors go deeper into the definition and consider that for the meaning of euthanasia, are necessary to consider elements that are essential in the word itself; such as the fact that it is an act that seeks to provoke death and that carried out to eliminate the suffering in the person who is dying. Other elements with a secondary character in the definition are the patient's consent (which must be granted respecting autonomy and freedom in the positive and negative sense; that means the fact must be not be coerced in any way). Another element is the terminal nature of the disease, with an irreversible outcome that generates precariousness and a loss of dignity. The third secondary element is the absence of pain of the death through the use of drugs such as high-potency analgesics, including opioids, high-potency muscle relaxants, and even anesthetic drugs. Finally, the last element is the health context in which the action is performed (essential in some legislations to be considered euthanasia) [ 10 ]. According to the World Health Organization, the union of these two components is the current definition of euthanasia, which describes as “the action performed by a person to cause the painless death of another subject, or not preventing death in case of terminal illness or irreversible coma. Furthermore, with the explicit condition that the patient must be suffering physical, emotional, or spiritual and that affliction is uncontrollable with conventional measures such as medical treatments, analgesics, among others; then the objective of euthanasia is to alleviate this suffering” [ 11 ]. Unfortunately, the term euthanasia has been misused over the years, and other practices have been named with this word. An example of this situation occurred during the Nazi tyranny when the word euthanasia concerned the murder of people with disabilities, mental disorders, low social status, or gay people. At that time, euthanasia was even a simultaneous practice to the Jewish genocide [ 11 ].
Not only has the term been misused; also exists an enormous variability of terms to refer to euthanasia. For example, the laws created to regulate euthanasia have different names around the world; in the Netherlands (Holland), the law that regulates this practice is known as the law of termination of life; in Belgium, it is called euthanasia law, in France, it is called euthanasia law too. In Oregon (USA), it is called the death with dignity act; in California, it is the end of life option act. In Canada is called the medical assistance in dying act. Victoria (Australia) is the voluntary assisted dying bill, but all these denominations refer to the already well-known term euthanasia [ 11 ].
3. Evolution of euthanasia and assisted suicide: digging into historical events
To understand the evolution and relevance of these concepts should analyze the history of euthanasia and assisted suicide; from the emergence of the term, going through its first manifestations in antiquity; mentioning the conceptions of great thinkers such as Plato and Hippocrates; going through the role of the Catholic Church; mainly in the Middle Age, where following the thought of St. Thomas Aquinas, self-induced death or death contemplated by own will, was condemned. Later, with the renaissance age and the resurgence of science, technology, and the arts, the term euthanasia made a transition to a form similar to what we know today from thinkers such as Thomas More and Francis Bacon. Finally, the first signs of eugenics were known in London, Sweden, Germany, and the United States in the twentieth century. There was a relationship with the term euthanasia that was later used interchangeably, especially in the Nazi regime, to denote a form of systemic murder that sought to eradicate those who were not worthy of living a life.
Since the sixties, with emblematic cases, the path towards the decriminalization of euthanasia began in some countries, especially concerning the cessation of extreme support measures in cases of irreversible illness or a terminal condition. The practice has progressed to the appearance of laws on euthanasia in several countries.
4. Euthanasia and assisted suicide in ancient times
In book III of Plato's “The Republic”, the author stated that those who live their lives amidst illnesses and medicines or who were not physically healthy should be left to die; implying that it was thought that people in these conditions suffered so much that their quality of life diminished, which seemed understandable to these thinkers. However, other authors such as Hippocrates and his famous Hippocratic oath sought the protection of the patient's life through medicine, especially in vulnerable health conditions prone to fatal outcomes. This Hippocratic oath is the same oath that permeates our times and constitutes an argument among those who mark their position against euthanasia and assisted suicide [ 12 , 13 ].
Other texts that collect thoughts of Socrates and his disciple Plato point out that it was possible and well understood to think of ceasing to live in the face of a severe illness; to consider death to avoid a long and torturous agony. This fact is compatible with the conception of current euthanasia since this is the end of this health care procedure [ 13 ].
In The Republic, the text by Plato, the physician Heroditus is also condemned for inventing a way to prolong death and over manage the symptoms of serious illnesses, which is currently known as distanasia or excessive treatment prolongs life. This kind of excessive treatment prolongs the sick person's suffering, even leading him to maintain biological signs present but in a state of alienation and absolute dependence on medical equipment such as ventilators and artificial feeding [ 13 ]. However, the strongest indication that Euthanasic suicide was encouraged in Greece lies in other thinkers such as the Pythagoreans, Aristotelians, and Epicureans who strongly condemned this practice, which suggests that it was carried out repeatedly as a method and was therefore condemned by these thinkers [ 12 , 13 ]. According to stoicism, the pain that exceeded the limits of what was humanly bearable was one of the causes for which the wise man separates himself from life. Referring to one of the nuances that euthanasia touches today, that is, at a point of elevated suffering, the dignity and essence of the person are lost, persisting only the biological part but in the absence of the person's well-being as a being. In this sense, Lucius Seneca said that a person should not love life too much or hate it; but that person should have a middle ground and end their life when they ceased to perceive life as a good, worthy, and longed-for event [ 1 , 12 ].
During the Roman Empire and in the territories under its rule, it was believed that the terminally ill who commit suicide had sufficient reasons to do so; so since suicide caused by impatience and lack of resolution to pain or illness was accepted, when there was no access to medicines. In addition, there was little development in medicine during that time, and many of the sick died without treatment [ 12 ]. This situation changed later with the emergence of the Catholic church; in this age, who attempted against own life, was deprived of burial in the ground. Saint Augustine said that the suicide was an abominable and detestable act; from 693 AD, anyone who attempted against his physical integrity was excommunicated. Rejecting to the individuals and their lineage, depriving them of the possibility of attending the funeral and even expelled from cities and stripped of the properties they owned [ 12 , 13 ].
4.1. Euthanasia and assisted suicide in the Middle Age
During the Middle Age, Catholicism governed the sciences, arts, and medicine; the sciences fell asleep. Due to this solid religious tendency and the persistence of Augustinian thought, suicide was not well seen. It was not allowed to administer a lethal substance to a person to end the suffering of a severe or terminal illness [ 9 , 12 ]. People who took their own lives at this time could not be buried “Christianly”; therefore, they did not have access to a funeral, nor to the accompaniment of their family in a religious rite. Physical suffering and pain were then seen as a path to glorification. Suffering was extolled as the form that god purified the sin, similar to the suffering that Jesus endured during his Calvary days. However, a contrary situation was experienced in battles; a sort of short dagger-like weapon was often used to finish off badly wounded enemies and thus reduce their suffering, thus depriving them of the possibility of healing and was called “mercy killing” [ 12 ].
5. Euthanasia in renaissance
With the awakening of science and philosophy, ancient philosophers' thoughts took up again, giving priority to man, the world, and nature, thus promoting medical and scientific development. In their discourse, Thomas More and Francis Bacon refer to euthanasia; however, they give a eugenic sense to the concept of euthanasia, similar to that professed in the book of Plato's Republic. It is precise with these phylosophers that the term euthanasia got its current focus, referring to the acceleration of the death of a seriously ill person who has no possibility of recovery [ 12 ]. In other words, it was during this period that euthanasia acquired its current meaning, and death began to be considered the last act of life. Therefore, it was necessary to help the dying person with all available resources to achieve a dignified death without suffering, closing the cycle of life that ends with death [ 13 , 14 ].
In his work titled “Utopia”, Thomas More affirmed that in the ideal nation should be given the necessary and supportive care to the dying. Furthermore, in case of extraordinary suffering, it can be recommended to end the suffering, but only if the patient agrees, through deprivation of food or with the administration of a lethal drug; this procedure must be known to the affected person and with the due permission of authorities and priests [ 12 , 13 ]. Later, in the 17th century, the theologian Johann Andreae, in his utopia “Christianopolis”, contradicts the arguments of Bacon and Moro, defending the right of the seriously ill and incurably ill to continue living, even if they are disturbed and alienated, advocating for the care based on support and indulgence [ 15 , 16 ]. Similarly, many physicians rejected the concepts of Plato, Moro, and Bacon. Instead, they focused on opposing euthanasia, most notably in the nineteenth century. For example, the physician Christoph Hufeland mentioned that the doctor's job was only to preserve life, whether it was a fate or a misfortune, or whether it was worth living [ 16 ].
5.1. Euthanasia in the 20th century
Before considering the relevant aspects of euthanasia in the 20th century, it is vital to highlight the manuscript by Licata et al. [ 17 ], which narrates two episodes of euthanasia in the 19th century. The first one happened in Sicily (Italy) in 1860, during the battle of Calatafimi, where two soldiers were in constant suffering, one because he had a serious leg fracture with gangrene, and the other with a gunshot wound. The two soldiers begged to be allowed to die, and how they were in a precarious place without medical supplies, they gave them an opium pill, which calmed them until they died [ 17 ]. The second episode reported by Licata et al. [ 17 ] was witnessed by a Swedish doctor named Alex Munthe; who evidenced the pain of many patients in a Parisian hospital. So he decided to start administering morphine to help people who had been seriously injured by wolves and had a poor prognosis; therefore, the purpose of opioid use was analgesia while death was occurring.
It is also important to highlight the manuscript entitled “Euthanasia” by S. Williams published in 1873 in “Popular Science Monthly”, a journal that published texts by Darwin, Edison, Pasteur, and Beecher. This text included the report for the active euthanasia of seriously ill patients without a cure, in which the physicians were advised to administer chloroform to these patients or another anesthetic agent to reduce the level of consciousness of the subject and speed up their death in a painless manner [ 16 ].
Understanding that euthanasia was already reported in the nineteenth century, years after, specifically in 1900, the influence of eugenics, utilitarianism, social Darwinism, and the new currents of thought in England and Germany; it began in various parts around the world, projects that considered the active termination of life, thus giving rise to euthanasia societies in which there were discussions between philosophers, theologians, lawyers, and medical doctors. Those societies discussed diverse cases, such as the tuberculous patient Roland Gerkan, who was considered unfit and therefore a candidate to be released from the world [ 16 ]. The scarcity of resources, famine, and wars were reasons to promote euthanasia as a form of elimination of subjects considered weak or unfit, as argued in texts such as Ernst Haeckel's. However, opponents to the practice, such as Binding and Hoche, defended the principle of free will in 1920 [ 16 ].
5.2. Euthanasia in the time of the Nazis
As mentioned above, the term euthanasia was misused during this period; approximately 275,000 subjects (as reported at the Nuremberg International Military Tribunal 1945–1946), who had some degree of physical or mental disability, were killed during Adolf Hitler's Euthanasia program [ 13 ]. However, the Nazis were not the first to practice a form of eugenics under the name of euthanasia, since the early 1900s in London had already begun the sterilization of the rejected, such as the blind, deaf, mentally retarded, people with epilepsy, criminals, and rapists. This practice spread to different countries like Sweden and the United States [ 13 , 16 ].
For the Nazis, euthanasia represented the systematic murder of those whose lives were unworthy of living [ 13 ]. The name given to this doctrine was “Aktion T4”. At first and by law, from 1939, the hospitals were obliged to account for all disabled newborns, which led to the execution of more than 5000 newborns utilizing food deprivation or lethal injection [ 12 , 18 ].
A year before that law, in 1938, one of the first known cases of euthanasia in children arose in Germany. That history called the story of child K, in which it was the father of the minor who asked Hitler in writing for euthanasia for his son because the child had a severe mental disability and critical morphic disorders. Hitler gave his consent to carry out the procedure on child K, and thus the program began to spread throughout the Aleman territory. Since then, physicians and nurses had been in charge of reporting the newborns with alterations, arising the “Kinderfachabteilugen” for the internment of children who would be sentenced to death after a committee's decision [ 12 , 18 , 19 ]. A list of diseases and conditions that were considered undesirable to be transmitted to Hitler's superior Aryan race was determined; thus, any child with idiocy, mongolism, blindness, deafness, hydrocephalus, paralysis, and spinal, head, and hip malformations were eligible for euthanasia [ 19 ].
Subsequently, the program was extended to adults with chronic illness, so those people were selected and transported by T4 personnel to psychiatric sanatoriums strategically located far away. There, the ill patients received the injection of barbiturate overdoses, and carbon monoxide poisoning was tested as a method of elimination, surging the widely known gas chamber of the concentration camp extermination; this situation occurred before 1940 [ 12 , 19 ]. Again, physicians and nurses were the ones who designated to the patients to receive those procedures; in this case, these health professionals supported Nazi exterminations. They took the patients to the sanatoriums, where psychiatrists evaluated them and designated with red color if they should die and with a blue color if they were allowed to live (this form of selection was similar in children) [ 12 , 13 , 19 ]. In this case, the pathologies considered as criteria for death were those generating disability such as schizophrenia, paralysis, syphilis with sequelae, epilepsy, chorea, patients with chronic diseases with many recent treatments, subjects of non-German origin and individuals of mixed blood [ 19 ]. Once in the sanatoriums, they were informed that they would undergo a physical evaluation and take a shower to disinfect themselves; instead, they were killed in gas chambers [ 12 , 13 ]. Despite the church's action in 1941 against Nazis and after achieving suspension of the Aktion T4 project; the Nazi supporters kept the practices secretly, resuming them in 1942, with the difference that the victims were killed by lethal injection, by an overdose of drugs, or left to starve to death, instead of the use of gas chambers. This new modified form of euthanasia, which did not include gas chambers, became known as “savage euthanasia” [ 12 , 13 , 19 ].
5.3. Euthanasia since the 1960s
In September 1945, trials began for crimes perpetrated by Nazi supporters; the victorious Allied forces conducted these trials at the end of the war. During these tribunals, cases of human experimentation were identified and the public exposure of the Nazi euthanasia program. After the Nuremberg trials and the abolition of Nazi experiments, a series of seven documents emerged, among which the Nuremberg code containing the ten basic principles for human research stood out [ 20 , 21 ].
After these judgments, biotechnology was accelerated, with the apparition of new techniques to intervene in the health-disease process. Additionally, the increase in life expectancy and the appearance of diseases that chronically compromise the state of health of people generated a change in the conception of the critically ill patient and the terminal state of life [ 20 , 21 ]. Cases such as Karen Ann Quinlan brought to the forefront the issue of euthanasia and precisely the control of extreme treatment measures. Karen, a young American woman, was left in a vegetative state due to severe neurological damage following alcohol and barbiturate intoxication. After six months in that state and under the guardianship of a Catholic priest, Karen's parents requested the removal of the artificial respirator, arguing that in her state of consciousness prior to the incident, she had stated that she disagreed with artificially maintaining life in comatose patients. The hospital refused to remove the ventilator, arguing the legal issues for the date, and the parents went to court, which in the first instance granted the hospital the right. Nevertheless, the New Jersey Supreme Court granted Karen Ann's right to die in peace and dignity. Despite the withdrawal of the artificial respirator, he continued to live until 1985, when he finally died [ [21] , [22] , [23] ].
Another important case was Paul Brophy, which also occurred in the United States. Paul was a firefighter in Massachusetts and went into a deep coma due to the rupture of a basilar artery aneurysm; initially, his family advocated for support measures but later requested the hospital to disconnect these means to allow death, as Paul had indicated when he was still conscious. The hospital refused to carry out this procedure, so the family went to court, where the removal of the support measures (gastrostomy) was initially denied. Hence, the family went to the state supreme court, achieving the transfer of Paul to another medical center where the gastrostomy was removed, leading to his death within a few days [ 23 ].
The case of Arthur Koestler, an influential English writer and activist diagnosed with Parkinson's disease and later with leukemia, who served as vice-president of the voluntary euthanasia society (Exit) and wrote a manual book with practical advice for euthanasia called “Guide to Self-Liberation”. He stood out because he applied one of his advice and ingested an overdose of barbiturates, causing his self-death. According to his writings, Koestler was not afraid of death but of the painful process of dying [ 23 ]. In this sense, it was a relevant case because it involved someone who held an important position in an association that advocated euthanasia, in addition to being the author of several works, which made him a recognized public figure [ 23 ].
Baby Doe was a case that also occurred in the United States; it was a small child with Down syndrome who had a tracheoesophageal fistula and esophageal atresia; in this case, surgery was necessary. On the advice of the obstetrician, the parents did not allow surgery, so the hospital managers took the case before a judge who ruled that parents could decide to perform or not the surgery. The case was appealed before a county judge who upheld the parents' power to make the decision, in the course of which the case became public and many families offered to take care of the child; however, before the case reached the supreme court, the child died at six days of age [ 23 ].
In the case of Ingrid Frank, a German woman who was in a quadriplegic state by a traffic accident, who initially sought rehabilitation but later insisted on being allowed to die; it was provided with a drink containing a cyanide solution that she drank. At the same time, she was filmed, which shows a kind of assisted suicide. For that reason, this is another case that deals with this issue and is important to know as background in the development of euthanasia and assisted suicide [ 22 , 23 ].
6. Current and future perspectives
The definition of brain death, the rational use of the concept of euthanasia and assisted suicide, and scientific literacy are the objectives of global bioethics to regulate euthanasia and assisted suicide, which can be accessible in all health systems [ [24] , [25] , [26] , [27] , [28] , [29] , [30] ]. End-of-life care will continue to be a subject of debate due to the struggle between biomedical principles, the different existing legal frameworks, and the general population's beliefs. Medical education and preparation in the perception of death, especially of a dignified death, seems to be the pillar of the understanding of the need to develop medical-legal tools that guarantee the integrity of humans until the end of their existence [ 31 , 32 ]. This is the reason why the new generations of physicians must be trained in bioethics to face these ethical conflicts during the development of their professional careers.
In addition, although the conception of bioethics belongs to the Western world, it is crucial to take into account the point of view of other cultures and creeds, for example, a study carried out in Turkey, where nursing students were questioned, found that many of them understood the reasons for performing euthanasia; however, they know that Islam prohibits it, as well as its legislation, and therefore they would not participate in this type of procedure [ 33 ]. Furthermore, Christianism and Islam prohibit euthanasia, but Judaism also prohibits it; in general, the so-called Abrahamic religions are contrary to any form of assisted death, whether it is active euthanasia, passive, or assisted suicide [ 34 ].
7. Conclusiones
The history and evolution of euthanasia and assisted suicide have been traumatic throughout human history. The church, politics, and biomedical research have been decisive in defining these concepts. Over the years, the legal framework and bioethical concepts on euthanasia have been strengthened. However, there is still much work to educate the general population and health professionals about end-of-life care and dignified death.
It is also important to remember that life is a concept that goes beyond biology. Currently, bioethics seeks to prioritize the concept of dignity, which must be linked to the very definition of life. Although the phrase is often heard that it is not necessary to move to be alive, what is important is that person feels worthy even if they have limited movement. The person's treatment must be individualized in bioethics since each individual is a unique unit. Therefore, medical paternalism must be abandoned. Instead, the subject must be more involved to understand their context and perception of life and dignity.
Ethical approval
It is not necessary.
Sources of funding for your research
Author contribution.
All authors equally contributed to the analysis and writing of the manuscript.
Provenance and peer review
Not commissioned, externally peer reviewed.
Research registration Unique Identifying number (UIN)
- 1. Name of the registry: Not applicable.
- 2. Unique Identifying number or registration ID: Not applicable.
- 3. Hyperlink to your specific registration (must be publicly accessible and will be checked): Not applicable.
Sabrina Rahman. Independent University, Dhaka, Bangladesh. [email protected] .
Declaration of interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
IMAGES
VIDEO
COMMENTS
The word Euthanasia is taken from a Greek word meaning "good or happy death". Narrowly speaking it is equivalent to killing so in these terms if allowing a person to die is not killing than its not euthanasia. By considering this we can conclude that allowing someone to die can be moral but killing someone which comes under euthanasia is wrong.
Why Active Euthanasia is Morally Wrong. Active euthanasia will promote the development of a society that gives priority to economic returns over individual freedom. A major concern is that many medical decisions are financial as well and as such, active euthanasia might be abused out of financial considerations.
Get custom essay. All the same, to some people's view it will be morally wrong to use euthanasia to terminate somebody's life even in whichever condition (Moreland, 2000). To these opponents of mercy killing, the problem arises because the approach focuses on happiness versus suffering and puts them at the forefront of life itself.
Religious arguments. Euthanasia is against the word and will of God. Euthanasia weakens society's respect for the sanctity of life. Suffering may have value. Voluntary euthanasia is the start of a ...
Some people are skeptical that <i>any</i> euthanasia request is truly autonomous, given the suffering and vulnerability that motivated the request. But most think that, as long as the doctor takes proper precautions to ensure the request is competent and voluntary, they can carry it out. And given the details of Jack's case, it seems ...
Persuasive Essay Pro Euthanasia Essay. Imagine facing a terminal illness with no hope for recovery, only prolonged suffering and pain. In such situations, the concept of euthanasia, or assisted suicide, becomes a controversial but increasingly relevant topic.
A slight majority of the physicians (56, 8%) believe that active euthanasia is ethically unacceptable, while 43, 2% is for another solution (35, 2% took a viewpoint that it is completely ethically acceptable, while the remaining 8% considered it ethically acceptable in certain cases). From the other side, 56, 8% of respondents answered ...
The Netherlands was the first country to allow legal euthanasia and assisted suicide in 2002, totaling 1.7-2.8% of total deaths. Euthanasia is generally illegal in the United States, but in a nationwide 2017 American poll, 73% of the public were in favor of euthanasia, and 57% said euthanasia is morally acceptable. These numbers are nearly ...
The impact of characterizing euthanasia as 'medical treatment' on physicians' professional identity and on the institutions of medicine and law should be examined in jurisdictions where assisted suicide and euthanasia have been de-criminalized. euthanasia, assisted suicide, palliative care, suffering, healing, medical legislation. Topic:
Indiana State University Abstract. All over the world, there is discussion being made about euthanasia and if it is ethically and. morally acceptable. The opinions are different from state to state and country to country. These. differences in opinions evolve from different religions, political forces, generations, genders, and. social classes.
Palliative Care. Physician Obligation. Financial Motivations. 1. Legalization. "The right to die should be a matter of personal choice. We are able to choose all kinds of things in life from who we marry to what kind of work we do and I think when one comes to the end of one's life, whether you have a terminal illness or whether you're ...
The word euthanasia, originated in Greece means a good death 1.Euthanasia encompasses various dimensions, from active (introducing something to cause death) to passive (withholding treatment or supportive measures); voluntary (consent) to involuntary (consent from guardian) and physician assisted (where physician's prescribe the medicine and patient or the third party administers the ...
This essay reviews ethical arguments regarding voluntary euthanasia and physician-assisted suicide from a utilitarian perspective. I shall begin by asking why it is normally wrong to kill an innocent person, and whether these reasons apply to aiding a person who, when rational and competent, asks to be killed or given the means to commit suicide.
Here are some examples of euthanasia essay topics and titles we can suggest: The benefits and disadvantages of a physician-assisted suicide. Ethical dilemmas associated with euthanasia. An individual's right to die. Euthanasia as one of the most debatable topics in today's society.
In the United States, physician-assisted suicide or aid in dying has always been carefully distinguished from euthanasia. Euthanasia, also called mercy killing, refers to the administration of a lethal medication to an incurably suffering patient. It may be voluntary (the patient requests it) or involuntary. Euthanasia is illegal in the United ...
The ethics of euthanasia is based on dualistic anthropology and wrong moral presuppositions underlying the defence of euthanasia, namely, proportionalism and consequentialism. The basic claim of proponents of the ethics of euthanasia is that human persons are consciously experiencing subjects whose dignity consists of their ability to made ...
Abstract. In discussions about the legalisation of active, voluntary euthanasia it is sometimes claimed that what should happen in a liberal society is that the two sides in the debate "agree to disagree". This paper explores what is entailed by agreeing to disagree and shows that this is considerably more complicated than what is usually ...
Why Euthanasia is Wrong Essay. "Thou Shalt Not Kill" (Exodus 20: 13-14). One of the Ten Commandments put forward by God to Moses at the top of Mount Sinai. The killing of another human being is morally wrong and unacceptable. No one has the right to take away another persons life, whether it be through hatred and disgust, or compassion and ...
Euthanasia Is Wrong Essay. The act of Euthanasia in humans today is one of the biggest and most controversial topics throughout society today. Euthanasia is defined as the act of taking a person's life, which is wrong even if the person desires to die. Voluntary euthanasia is when the person who is killed has requested to be killed.
Reason #4: Allowing Euthanasia Makes True Palliative Care Worse. Euthanasia is, by its nature and definition, in complete opposition to the principle of "do no harm.". Thus, euthanasia and palliative care are completely incompatible. Palliative care seeks to provide dignity, comfort, and compassion in a person's final days.
3. Evolution of euthanasia and assisted suicide: digging into historical events. To understand the evolution and relevance of these concepts should analyze the history of euthanasia and assisted suicide; from the emergence of the term, going through its first manifestations in antiquity; mentioning the conceptions of great thinkers such as Plato and Hippocrates; going through the role of the ...
Rachels uses the theory of utilitarianism in his article titled The Morality of Euthanasia. The first part of the theory, developed by Jeremy Bentham, explains how morality is based on two elements: happiness and misery. If something is deemed morally wrong, it decreases happiness and increases misery.